

The popular VAERS "deep dive" is quite shallow
Truth in Numbers (Daniel) on Twitter posted a widely shared VAERS "deep dive" thread, but it has all the usual blind spots that affects the analysis of the vaccine pushers

Summary:
A widely shared VAERS “deep dive” Twitter thread by Truth in Numbers (Daniel) is almost completely wrong in its conclusions
This happened because he used a small sample of 120 reports out of a total of 16K+ US VAERS death reports
This is a problem of skillset deficit. Reading the writeups in VAERS reports at scale is only feasible if you can use some data science and Natural Language Processing techniques. And not just Daniel’s, but most VAERS analysis I have seen do not use these techniques
More worryingly, the people in the tech community who do have these skillsets completely ignore vaccine injury datasets1
As a result, there are a LOT of blind spots in Daniel’s analysis. I list ten of these blind spots in this article, but there are probably many more.
This is the VAERS thread I am talking about:
The first thing we should “get out of the way”, so to speak, is that claiming “VAERS is a valid measurement tool” is very different from claiming that the existing VAERS data is being ignored by the CDC.
Update 24th Jan 2023:
Why do I think CDC is ignoring VAERS data?
Because they could have easily used VAERS to cross-verify claims made by Pharma companies, and they never did. For example, I wrote an article recently about how I used VAERS as a checksum to demonstrate that Pfizer had undercounted myocarditis vaccine injuries when it submitted its pharmacovigilance plan report to the FDA in mid-July 2021As far as I can see, most VAERS analysts claim the latter and not the former. In other words, you can agree that VAERS is not a valid measurement tool, but also use it to cross-verify other information provided by Pharma companies and the health regulators.
If the vaccine is offered as the only solution2 during a pandemic, this kind of open-source data scrutiny must be encouraged by the health regulators.
In fact the deep dive from Daniel itself helps me make this case, as I will show you in this article.
Finding all the reports by age
This is the second tweet:

Blind Spot #1: As best as I can see, most vaccine pushers are not even aware of the existence of foreign VAERS reports
The age is missing from a large majority of foreign reports, even though the age is clearly mentioned in the writeup:
Why is the age field missing in so many foreign VAERS reports?

A few days back, the founder of OpenVAERS made an interesting point on Twitter
In turn, this means there isn’t any way to find all the reports under a certain age. At best you will get a subset, which means your analysis will be cherry-picked.
And if you had read the foreign reports, you would know that this problem also exists in the US VAERS dataset, on a much smaller scale.
To prove this, I ran the following query on my combined_vaersdata3 CSV file:

As you can see, there are 374 death reports in US VAERS where the age is missing, but the text writeup includes the words ‘year’ and ‘old’.
As you can see, there are also some death reports which do not include the age even for children.
For example, here is a VAERS death report for a 13 year old boy who died three days after COVID vaccination, and which is missing the AGE field. Daniel’s analysis would have omitted this, even though the report is not fake.

Blind Spot #2: Vaccine pushers are not aware that a lot of VAERS death reports do not translate all the fields into the CSV file, even though the information is clearly mentioned in the text writeup. We should not omit such reports from the analysis.
You cannot make strong assertions about incomplete data
If you read all the 374 reports I have listed above, you will notice that they do not all have age information included. The ones which don’t provide the age would be the “false positives” - i.e. even though they do not mention the age in the writeup, the SQL query will still select them because they satisfy the query rules.
Now, it might seem like I am arguing against my own position here, but I am simply arguing for more scrutiny of the dataset.
For example, let us filter the dataset to select only the reports which include the text ‘unknown age’

Here is the full writeup for the highlighted VAERS report (emphasis mine)
Died the next day; This spontaneous case was reported by a consumer and describes the occurrence of DEATH (Died the next day) in a female patient of an unknown age who received mRNA-1273 (Moderna COVID-19 Vaccine) for COVID-19 vaccination. No Medical History information was reported. In December 2021, the patient received third dose of mRNA-1273 (Moderna COVID-19 Vaccine) (unknown route) 1 dosage form. Death occurred on December 2021 The patient died in December 2021. The cause of death was not reported. It is unknown if an autopsy was performed. No concomitant medications were provided. No treatment medications were reported. The patient took the booster shot about 4 days ago and died the next day. The paramedics found the patient sitting upright dead with an oxygen mask on. This fatal spontaneous case concerns an unknown year-old, patient with no medical history who experienced the unexpected fatal events of DEATH The event occurred unknown days after third dose of Moderna Covid 19 vaccine. The cause of death was not reported. It is unknown if an autopsy was performed. The rechallenge is not applicable The benefit-risk relationship of mRNA-1273 vaccine is not affected by this report.; Sender''s Comments: This fatal spontaneous case concerns an unknown year-old, patient with no medical history who experienced the unexpected fatal events of DEATH The event occurred unknown days after third dose of Moderna Covid 19 vaccine. The cause of death was not reported. It is unknown if an autopsy was performed. The rechallenge is not applicable The benefit-risk relationship of mRNA-1273 vaccine is not affected by this report.; Reported Cause(s) of Death: Unknown cause of death
As you can see, the patient’s age is not mentioned anywhere in this writeup, but this report still got selected by my SQL query because it does include both the words ‘year’ and ‘old’
The reason I include this example is because it is very hard to make strong assertions about an incomplete dataset like VAERS.
This goes both ways, meaning automated text analysis of the VAERS writeups will produce false positives and false negatives.
But most of these false results can be avoided using improved text Machine Learning algorithms, and probably even more with large language models like ChatGPT.
Why did the tech community turn such a blind eye towards VAERS?
Blind spot #3: Are the vaccine pushers even aware that the tech community has paid no interest4 to this topic? Also, how did the ENTIRE tech community avoid doing any serious text analysis of the VAERS dataset for nearly three years?
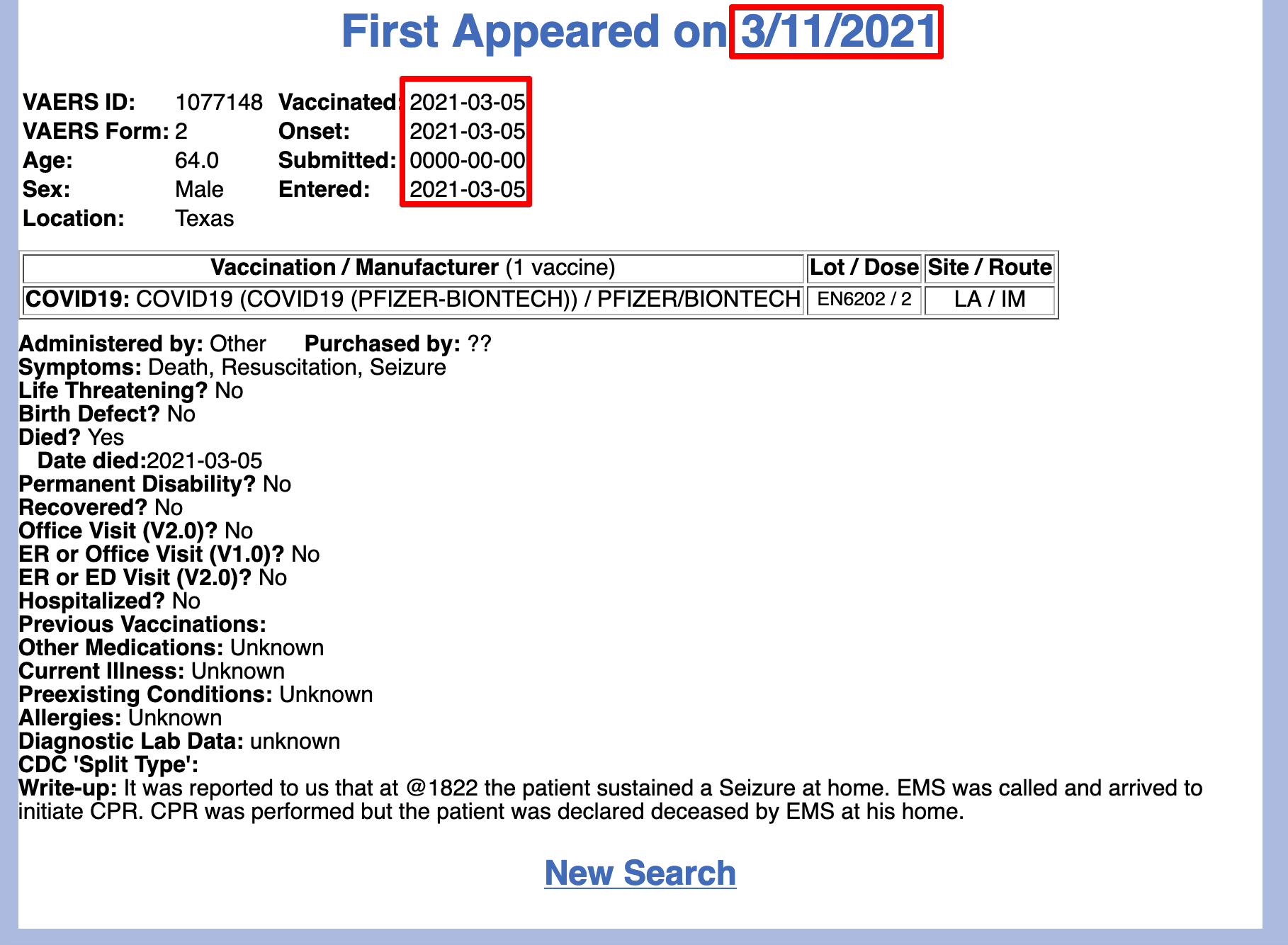
Were 61% of deaths from or with COVID?
These are the next three tweets in that thread:
At first, I wasn’t sure how Daniel came to this conclusion that 61% of reported deaths in VAERS were from or with COVID.
But he himself explains it in a different tweet:

First of all, he only looked at about 120 death reports (by his own admission later in the same thread) out of a total of 16000+.
This is less than 1% of all the death reports.
While I agree that reading 100 plus death reports is very time consuming, that does not really make it a “large sample”. But more importantly, depending on the earliest and latest value of the RECVDATE in Daniel’s sample, the entire analysis could be distorted.
I suggest Daniel publish all the 120 VAERS IDs if he wants people to actually believe his conclusion about 61% of VAERS deaths being “with or from COVID19”
But we can go a little further than that: if we look at the cause of death in foreign VAERS, we see that COVID-19 and associated symptoms makes up less than 20% of all the death reports.
Let us use my serious foreign VAERS reports search tool.
First select OUTCOME as Death. There are 16792 deaths as of November 20225.

Then select all symptoms related to COVID19 from the SYMPTOMS list.
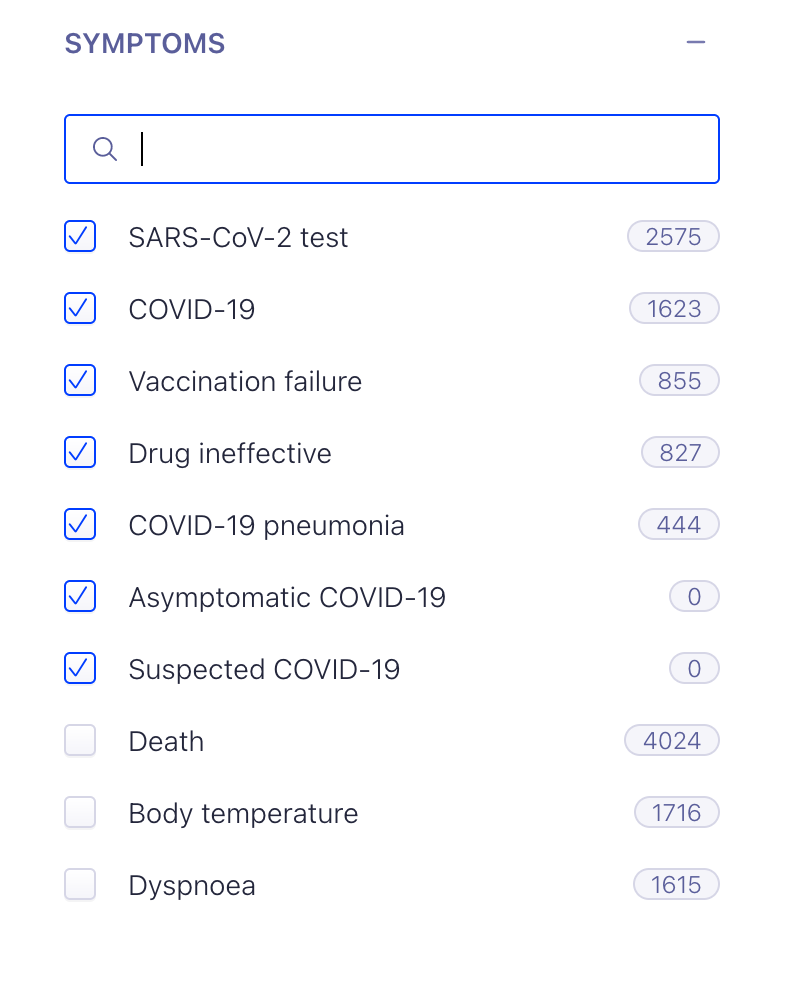
Note that I used the “Drug Ineffective” and “Vaccination Failure” symptoms which were mentioned in Pfizer’s own pharmaco-vigilance plan report to the FDA.

There are still only 3265 deaths after including all of these symptoms.

This means only 3265/16792 = 19.5% of the foreign VAERS death reports were from or with COVID-19.
While the general health of the US and foreign population is quite different, I very much doubt it is so different as to cause a 3X difference in outcomes (61% versus 20%).
Note: I started doing some analysis to extract the reported cause of death from VAERS writeups for foreign death reports and published it as Part 1 a while back. It was in preparation for doing the same analysis for the US VAERS death reports. Now that I have learnt that the 61% number claimed by Daniel is based on a sample and not on the entire dataset, I don’t intend to publish Part 2 (based on US VAERS death reports) until Daniel publishes all the 120 VAERS IDs he analyzed.This is the next tweet in that thread, and I have already shown that it is false.

Blind Spot #4: As you can see, breakthrough COVID is DEFINITELY not “driving most reported deaths” in foreign VAERS. Vaccine pushers are incorrect about this at least with respect to foreign VAERS. As for the US, I will wait for Daniel to publish the IDs for the 120 reports he has read before writing my rebuttal.
Who files VAERS reports in the US?
Here are the next two tweets in that thread:

I at least partly agree with Daniel here, as I have also seen that a large majority of US VAERS reports are not filed by healthcare professionals.
Identifying REPORTER field from the writeups of serious VAERS reports

People may not know this, but VAERS actually collects a lot of information about the person who files the report. But they don’t publish the information collected within the checkboxes. (To the best of my knowledge they don’t even provide aggregate information about the Reporter checkbox, if I am wrong please leave a comment).
On the other hand, foreign VAERS reports are the exact opposite of what Daniel points out:
a) they do contain a lot of medically relevant information
b) there are almost no anti-vaxx diatribes
Not only that, we already know from a paper written by the CDC itself, that nearly 100 percent of foreign VAERS reports are filed by the vaccine manufacturer, after they are adjudicated to be both serious and unexpected.
During 2011-2014, VAERS averaged around 30,000 U.S. reports annually, with 7% classified as serious. Healthcare professionals submitted 38% of reports, vaccine manufacturers 30% and patients and parents 14%. Reporter type and percent of serious reports vary across vaccines, age of vaccine recipient and how long the vaccine has been in use. During this same time period VAERS averaged around 6,000 foreign source reports annually. Vaccine manufacturers, which accounted for >99% of foreign source reporting, are required by law to submit foreign source adverse event reports that are both serious and unexpected [21], but not other types of foreign source reports. Given the vaccine manufacturer reporting requirements and the minimal amount of direct public reporting, it is not surprising that a relatively high percentage (48%) of foreign source reports are classified as serious. This likely represents selective reporting based on regulatory requirements rather than any substantial differences in safety profiles of foreign vaccines
Given all this, isn’t it very strange that there is such little scrutiny of foreign VAERS reports?
Why are foreign VAERS reports not being scrutinized by journalists?

Summary: A recent article about active surveillance of Myocarditis and Pericarditis reports from Australia mentions that their health regulator was unaware of these side effects until May 2021, and downplayed the risks even after they became aware From reading the pharmacovigilance documents submitted to the FDA
In fact, I would even go so far as to say that for almost every insight you can infer from doing text analysis of foreign VAERS writeups, there isn’t enough information to do that exact same type of analysis in US VAERS writeups.
Blind spot #5: Vaccine pushers do not seem to know the utility of foreign VAERS data as a means to cross-verify US VAERS analysis
The big problem of followup reports
The next tweet in the thread is most interesting for me, because it actually highlights a major problem in the VAERS followup process.

First of all, even though Daniel did not reveal the IDs of these two reports, let me acknowledge that there are probably quite a few examples of this.
But what he may not know - these are usually not repeated filings for the same vaccine injury just to clog up the system. Rather, this is usually someone trying to update an old VAERS report with additional information.
Most people who dismiss VAERS analysis are not even aware of the number of hoops someone must jump through to add updates to an existing VAERS report. This process has now been thoroughly documented to be very challenging for laypeople
Some victims had basically filed initial reports 3-4 times via themselves and their physicians. Many victims were getting wrong info from their physicians, because many physicians assumed filing follow-up data was the same process and submitting an initial report. IT IS NOT! There is a method of submitting follow-up data that requires a activation key# being submitted to you first, and a different portal access expressly for this purpose. This observation covers the victims that had since died or became permanently disabled but wanted their public facing initial report to reflect the current status.
After noticing this, the CDC decided to delete followup reports filed using a new VAERS ID. While their justification for doing this is to avoid “duplicate” reports in the system, it has caused its own set of problems as one would expect.
In the most extreme cases, if someone files a VAERS report upon being hospitalized, and then dies from the injury, their initial report does not reflect the fact that they died.
How the VAERS followup process hides death reports

Someone left this comment on my previous article: Only publishing initial reports begs the question, how many people are now since dead in VAERS? It is a non-zero number, meaning anyone who is using VAERS to analyze this information is certainly undercounting the total number of deaths.
In general, these VAERS deletions remove a big chunk of useful information from the public facing search.
This means even the people who are poring over individual VAERS reports and doing diligent analysis are still missing the full picture. While I don’t think there is anything nefarious about VAERS deletions, and I have stated exactly that many times on this website, they are still a big problem.
VAERS deletions are not nefarious

Jessica Rose recently shared an article of mine (thanks!) about VAERS deletions. A warm welcome to all my new subscribers! I will state up front that I don’t have much bandwidth to moderate even the few comments I receive, and prefer to focus my spare time on the vaccine data analysis. So I would very much appreciate it if the comments are focused on th…
Blind spot #6: most vaccine pushers are not aware of the challenge of updating existing VAERS reports, or the fact that the followup reports with new VAERS IDs are deleted from the public facing search engine
Did clearly healthy people die after taking the vaccines?
These are the next two tweets in the thread:
This is one of those arguments which you can refute by parsing the text writeups (note: some of the results would be false positives) to see if it mentions that any clearly healthy people died after taking the vaccines.
There were about 500 such reports.
Did clearly healthy people die from the mRNA vaccines?

Summary: There are over 500 death reports in foreign VAERS where the writeup includes a keyword which suggests the patient was healthy Some of these are false positives, but only a small percentage There are over 100 death reports where the symptom onset was on the same day of the vaccination
As you can see, there were also a few children in the 12-15 age group in that list.

Here are the VAERS reports for the screenshot above:
https://medalerts.org/vaersdb/findfield.php?IDNUMBER=2404821&WAYBACKHISTORY=ON
https://medalerts.org/vaersdb/findfield.php?IDNUMBER=2323471&WAYBACKHISTORY=ON
https://medalerts.org/vaersdb/findfield.php?IDNUMBER=2141783&WAYBACKHISTORY=ON
https://medalerts.org/vaersdb/findfield.php?IDNUMBER=1862946&WAYBACKHISTORY=ON
Blind spot #7: vaccine pushers seem to think every post-vaccine death was someone who was clearly in poor health. This is simply not true.
How many people died from “breakthrough COVID19”?
This is the next tweet:
In case you were not aware, apparently Pharma had already coined the term “breakthrough pain” in the Oxycontin case.
In fact, this has now turned into a meme on Twitter.
As I mentioned in a previous paragraph, Pfizer was initially tracking breakthrough COVID19 cases in their pharmacovigilance reports.
The Preferred Terms were “Drug ineffective” and “Vaccination failure”
If you filter for these in the foreign reports search tool, you only get 1678 deaths. This is just 10% of all the deaths in foreign VAERS.
Why are US VAERS reports so sparse?
These are the next two tweets:

While I agree with these observations, and think that the two things are probably related, there is one more factor we need to consider when asking why so many US VAERS reports came from consumers, while a large majority of foreign VAERS reports were done by healthcare professionals.
I think the reason for this has to do more with the US penalizing healthcare professionals who were reporting vaccine injuries.
While I don’t know how often this happened, the hospitals only needed to make an example out of a handful of people to make others more fearful of filing VAERS reports.

By the way, Gail Macrae recently gave an interview where she blew the whistle on this and other COVID topics.
This did not happen in other countries, and the result is that over 90% of foreign VAERS writeups are very detailed. As I mentioned before, they often do not translate the age field into the CSV column for some reason, but it is possible there is some simple bureaucratic reason for this.
Besides, you can still write a Python script to extract this age from the write up and use it for your analysis, as I have done in many previous articles.
Blind spot #8: The vaccine pushers don’t seem to even know that the US was disincentivizing healthcare professionals from speaking up about vaccine injuries.
Sudden Death reports in VAERS
These are the next two tweets:

I have already written about this topic, in fact it was based on these two tweets.
Sudden death reports in US vs foreign VAERS

Key takeaways: data scientists can construct a simple SQL query to find sudden cardiac death reports in VAERS there are about 300 sudden death reports in foreign VAERS and over 50 sudden death reports in US VAERS, and the foreign VAERS reports are qualitatively
I would also like to thank Daniel for making my point here.
After all, he has also accidentally proved that if someone reads less than 1% of the full list of death reports, there is a fairly good chance they will miss some important patterns which don’t happen very often6.
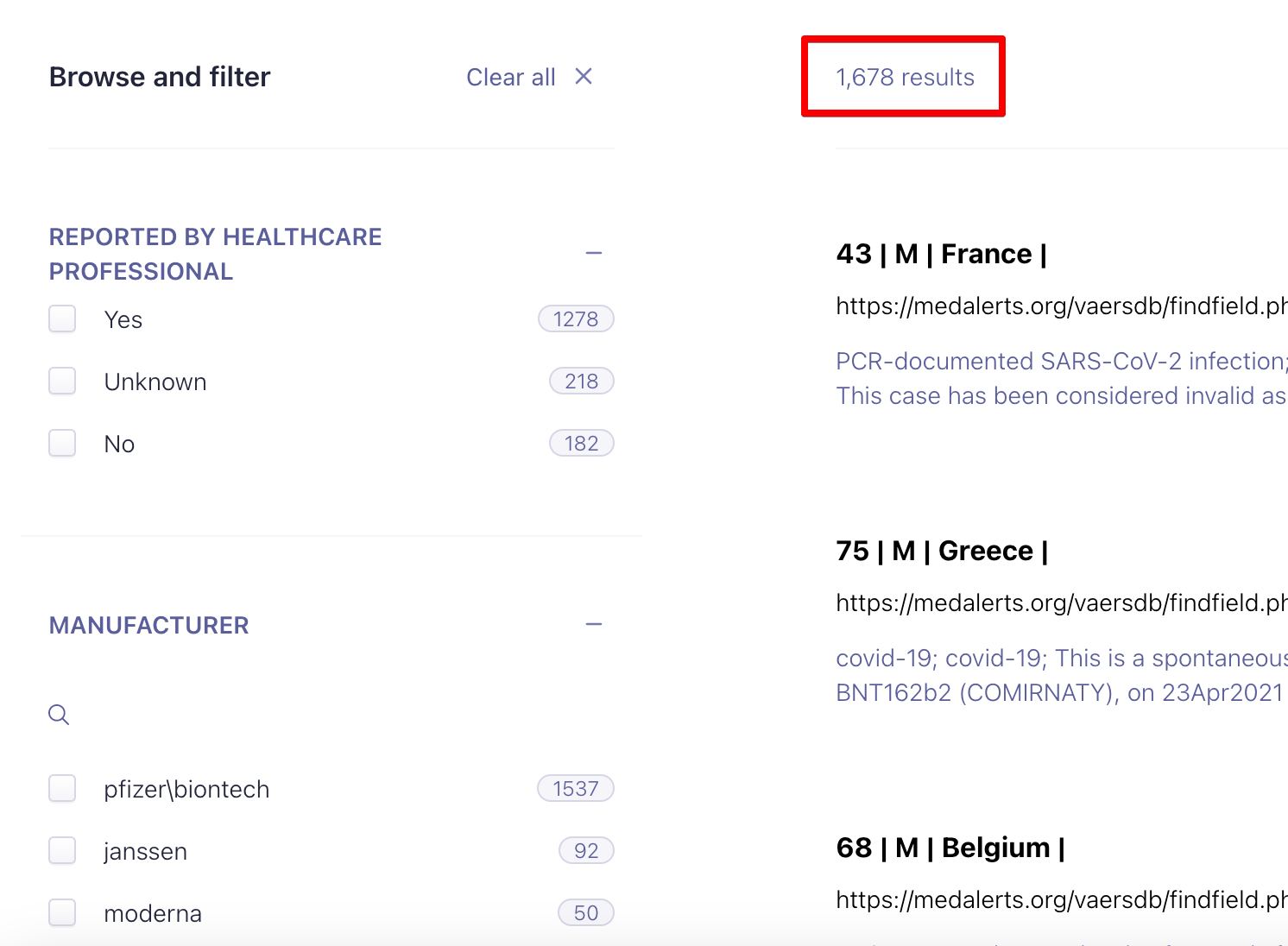
Median Age of deaths
This is the next tweet:
Apparently, someone’s refusal to obey COVID19 protocols could “kill grandma”, even though it is nearly impossible to know for sure how Grandma caught COVID.
However, the same Grandma can die after having symptom onset within one day of the COVID19 injection, and they will go “Oops! Looks like Grandma was too old and fragile for the ‘safe and effective’ vaccine!”
For example of the 8197 deaths of people over the median age of 75, 1135 had symptom onset within a day of being vaccinated. And about half of those also died almost right after symptom onset.

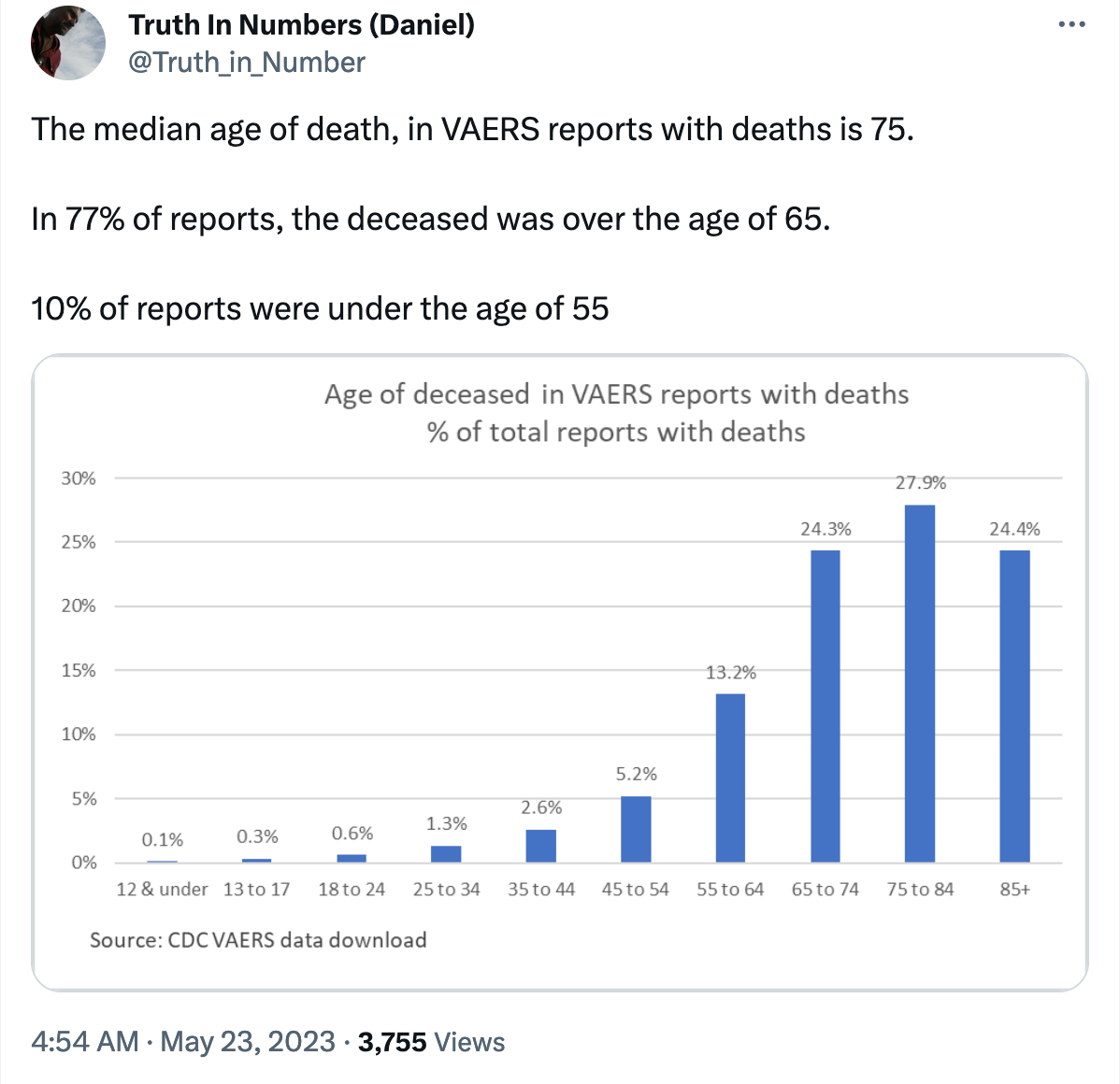
Same Day Deaths
This is the next tweet:

I am not sure what is so suspicious even if Daniel found “many” reports which had vaccination date, report date and death date as the same, given that the “published” date is the date the report goes public - and it is almost always a later date.
In fact, if the death date is the same as the vaccination date, the only thing I would actually be suspicious of is the claim that the vaccine is perfectly safe.
To do some further analysis, I first queried for the list of reports where the death date is the same as the vaccination date.

I found 357 such reports, which is roughly about 2% of the total number of death reports and matches what Daniel has stated.
Now let us filter by reports where vaccination date, report date and date of death are all the same.
Out of a total of 357 reports, only 43 of them satisfy this criteria.

Even for the reports which were received on the same day as the death date, you can see that the writeup mentions that the patient did, in fact, die soon after getting the vaccine.
But even in these cases, the published date is often different as you can see below.
The published date is not provided in the VAERS CSV file (which does make sense) and you need to open the report in the MedAlerts Wayback Machine to see when the report was first published.
As you can see, most reports are not published on the same day it was received.
In fact, Pfizer took advantage of this delay and was able to report far fewer cases of myocarditis in its pharmacovigilance report in mid-2021
98% of myo/pericarditis foreign VAERS reports were published after the PVP analysis

Summary: There were long delays between the date the report was received and the date it was actually published for a lot of foreign VAERS reports in early 2021 The usual explanation - that the system got overwhelmed because of too many reports - already reflects very poorly on the CDC because they had many months to anticipate and prepare
Blind spot #9: I very much doubt that the vaccine pushers understand the meaning and implications of the published date in the VAERS system.
The importance of using Natural Language Processing for VAERS analysis
Finally, we come to the place where Daniel mentions how many reports he actually read to do all his analysis.
But if you do not do any kind of automation (in terms of Natural Language Processing and text analytics), the limiting factor will always be the number of reports that you can manually read.
As I mentioned before, 120 reports is not even 1% of the total number of death reports for US VAERS. How much can you really infer from it?
And after providing a list of 10 sample reports he read, he concludes the thread with the following tweets:

But all this is still limited by the number of reports someone can manually read.
A human can perform much better at comprehending the writeup in the VAERS report than a machine - in fact a human will also perform better than the recent large language models like ChatGPT, in my opinion.
But if you have a dataset the size of VAERS (which now has over 1 million reports for the COVID19 vaccines), human effort alone will still be inferior to finding patterns using
a) large scale text analysis using Natural Language Processing (NLP)
b) large scale text analysis using NLP driven by7 human insight
For example, I recently wrote an article explaining how even some basic knowledge of data science is sufficient to notice that the “Grand Debunk” article on VAERS is almost entirely wrong.
The "Grand Debunk" is wrong about VAERS

Summary The “Grand Debunk” of the “Turtles” book on the Science Based Medicine (SBM) website is written by people who seem to lack basic data science skills v-safe free text information was not actively monitored, and you will know this if you had basic knowledge of Natural Language Processing
Another example is how none of the vaccine pushers have noticed that the CDC did not actually do any text mining of the unsolicited symptoms in the free-text responses from v-safe.
Peer Reviewed Lancet paper highlights CDC's v-safe text mining failures

Summary: A CDC paper published in August 2022 is the only one (I know of) which published sample verbatim free-text responses from v-safe The paper tries to filter free text responses related to menstruation, and to further classify them on different dimensions like severity etc. using a pretrained Machine Learning classifier
Blind spot #10: vaccine pushers don’t even know what they don’t know when it comes to NLP and text analysis.
Conclusion
Given that Daniel already has a background as a data analyst, he should probably spend a few weeks and learn the pandas library as well as the basics of the spaCy NLP library and repeat the same analysis he did, but using the foreign VAERS dataset.
I think his conclusions about VAERS could dramatically change if he does that.
Ironically, VAERS could in fact be one of the best datasets for training text Machine Learning algorithms for the medical domain because it already has a LOT of human annotated fields. In turn, this means we can mostly skip the training data generation step and accelerate the process of creating ML models.
Otherwise there would be no need for mandates
To run this query, you need to do some data preprocessing. You have to append each of the three CSV files (DATA, VAX, SYMPTOMS) for the years 2020 through 2023, and this is easiest to do using the pandas Python library
In case you are wondering, one of the things which would indicate interest is for a small team to create a highly specific machine learning model dedicated to VAERS reports. There are a lot of models like that for many other domains. For example, I used a general purpose off-the-shelf ML model for the biomedical domain (which was first published many years back, in fact) to prove that a very small fraction of VAERS reports would qualify as “crazy” reports.
Reminder, I am using the mid-November 2022 snapshot of the foreign dataset because the CDC stopped publishing the text writeups for the EU VAERS reports after that. I wonder if Daniel has the curiosity to ask the CDC if they are trying to hide something?
To push back against those who might ask “Why should we worry about something that did not happen very often?”, I think this is a key difference between the vaccine skeptics and the vaccine pushers. The goal should be to make vaccines safer and raise the standard for future vaccines, not to lower our expectations from them just so we can feel better about our past decision to take the vaccine.
In fact, this is the main benefit of data science. It helps people rapidly generate and test hypotheses which permit a fair percentage of false positives/negatives, and you can use the preliminary analysis as the starting point to then methodically eliminate the false positives/negatives if you want.
Given the purge of FR reports in nov 2022 if he were to learn and employ NLP, we should provide him that dataset... of course that will never happen. It has however been on todo list. We may hit you up at that point on a second dataset.
Some of the symptom entries I have regarded as vaccinated and got covid anyway (but these numbers are among all rather than just DIED):
215736 COVID-19
79561 Vaccination failure
74825 Drug ineffective
63262 SARS-CoV-2 test positive
8735 Vaccine breakthrough infection
8186 COVID-19 pneumonia
3726 Exposure to SARS-CoV-2
3293 Asymptomatic COVID-19
549 Breakthrough COVID-19
101 Occupational exposure to SARS-CoV-2
457,974 Total
... over at https://deepdots.substack.com/p/85-are-serious-in-vaers-reports-not ... 85% are Serious in VAERS Reports, NOT 20%, Study Reveals
The reason I mention it here is it came to mind while digging into Aravind's search tool at the mention above around "This means only 3265/16792 = 19.5%" and because I'm not totally certain my list is really all of ==> Got vaxxed but then got covid anyway <== [Let me think for a moment, what was that about effective? I digress]
... or that there aren't even more while not tagged with any of those by CDC.
Others might just mention in the writeup different things like ... Patient has covid, or does have covid or has contracted covid ... etc .... on-and-on, without any of those official tags added.
To a casual reader, it's an illustration of how difficult this work is because of data inconsistency and as we see so thoroughly, variations in wording. A report that coincidentally happens to be on the screen in front of me, just to highlight the point ( 2001383 ) DOES HAVE a couple of those entries, and DIED changed back and forth by the way between Yes and No ... Positive COVID-19 PCR on 12/27/2021,"Per System, patient received 2 doses of Pfizer COVID-19 vaccines on 7/26/2021 and 8/16/2021 and was subsequently diagnosed with COVID-19 at our hospital on 12/27/2021", ... _|_COVID-19_|_SARS-CoV-2 test positive_|_
The "Positive COVID-19 PCR on 12/27/2021" is in LAB_DATA, a field that doesn't receive a lot of notice. For some purposes I search all fields at once using the flat file: https://deepdots.substack.com/p/new-vaers-flat-file-easy-data-mining
There ought to be millionaires stepping forward to each transfer something like $50,000 a year to people like Aravind along with all the others doing significant work in this area.