

Is the ICAN v-safe lawsuit a "scam"?
Debunk the Funk's video is what happens when third rate vaccine safety standards meet a large skillset deficit

I recently subjected myself to this video, where “Debunk the Funk” Dr Dan Wilson claims that ICAN’s lawsuit to get CDC to publish v-safe free text entries is a “scam”.
I will add the following disclaimers before I explain why I think Debunk The Funk is wrong on this topic.
In my opinion, the v-safe free text data does not categorically prove that the mRNA vaccines are unsafe. We need to see the full text data to be able to confirm this, and that will only happen by early 2025.
There is still some analysis which I need to do to fully explain what I am saying in this article. I will do the analysis and write it up over the next few weeks.
I used my AudioJots software to generate a skimmable1 transcript of Dan Wilson’s video.

Why ICAN and CHD increased their revenues after the COVID19 vaccination
So let me address the first thing
One of these biggest groups is the informed consent Action Network, abbreviated ICANN, and their associated talk show with someone who I've talked a lot about on this channel before, Dell Bigtree. And these groups have been flourishing since the COVID pandemic started. ICANn specifically has increased its revenue by 60% in 2020, bringing it to $5.5 million in revenue. And those profits have increased since then. Most of this money comes from private donors, but these profits dont include speaking fees and ad revenue that they make through their talk show.
@00:01:01: Just a side note, Robert F. Kennedy junior s anti vaccine organization more than doubled its revenue in 2020, bringing in a total of $6.8 million. But this video is about ICANN and Dell Bigtree because they are currently misrepresenting the results of another frivolous lawsuit that they expect to make them big bucks. And the whole way they present the results of this lawsuit requires them to lie to you. And that's what I'm going to cover in this video. Hey, I'm doctor Wilson. I'm a PhD molecular biologist. And welcome to another debunking video.
This is a good example of how the vaccine pushers want to have their cake and eat it too.
When we ask -
“Why are there so many VAERS reports for the COVID19 vaccine?”
They say :
“Oh that’s because we injected so many people this time, which has never been done before”
Then why don’t they extend the same logic to the number of people who might potentially be injured by the vaccine and are now looking for answers?
Isn’t that enough to explain the jump2 in revenue?
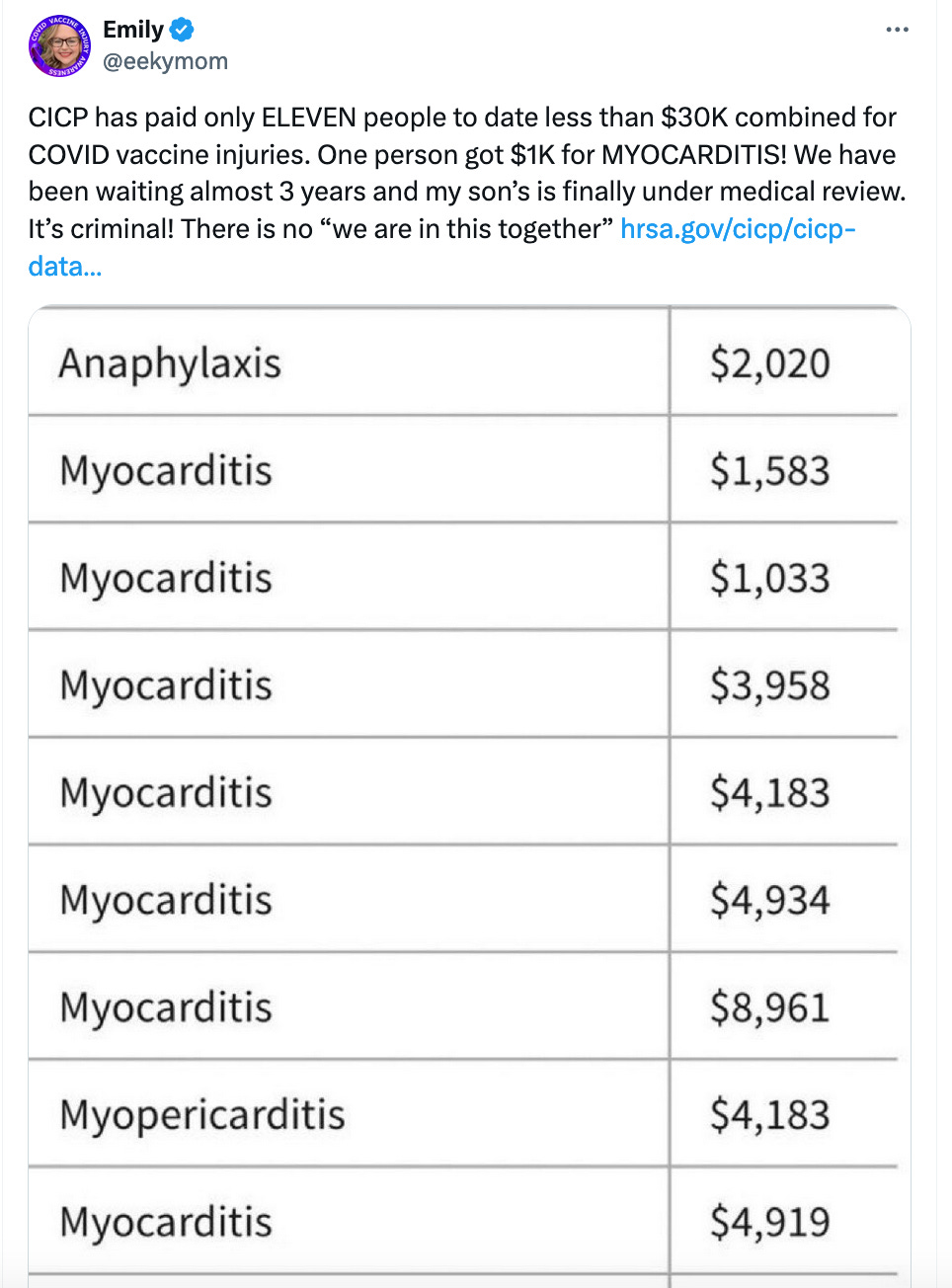
And of course, the situation is made even worse in the US because their CICP program has barely paid out any compensation for the COVID19 mRNA vaccines.
So who is going to fight on behalf of those people who believe they sustained a vaccine injury?
And what exactly does Debunk think would happen if all the vaccine injury discussion was censored3?
Occam's Eraser

Note: I normally don’t prefer to write these types of articles which just aggregate a lot of information but don’t get into much technical analysis. There is probably very little I am adding to the discussion which COVID19 vaccine skeptics don’t already know, plus for some reason these take much longer for me to write.
Here is what will happen - only those who already have a large donor base will be able to resist this kind of censorship, creating a winner-take-all effect.
I think that’s the main reason for CHD’s and ICAN’s jump in revenue.
Can we learn NOTHING new from the v-safe free text data?
Then Debunk goes on to say this4:
But Dell Bigtree and his lawyer say, no, no, no, we don't have the whole story because people sign up with this app and they share confidential patient information. Not all of the information that was received by VSafe is public due to HIPAA laws. In case you don't know, HIPAA laws protect patients confidential health and personal information. So what did ICANN do? They sued the CDC so that they could release redacted full files on what the VSafe participants submitted. This includes a text box where they could add additional comments for whatever they're experiencing.
@00:03:01: What do we expect to learn from reading these text boxes? Well, nothing, since all of the research currently published about V safe and all of the other vaccine safety reporting systems, again, not just from America, but from all over the world, include medical history, follow up with physicians, autopsies, and epidemiological investigations. There's absolutely no good reason to expect that text boxes in a messaging app are going to teach you anything new.
That last highlighted sentence is a good example of a third rate safety standard.
Even if every other type of analysis showed that the COVID19 vaccines were safe, it is absolutely necessary to analyze every piece of available evidence to confirm that.
I cannot believe anyone, let alone an actual medical professional, would be so casual about this!
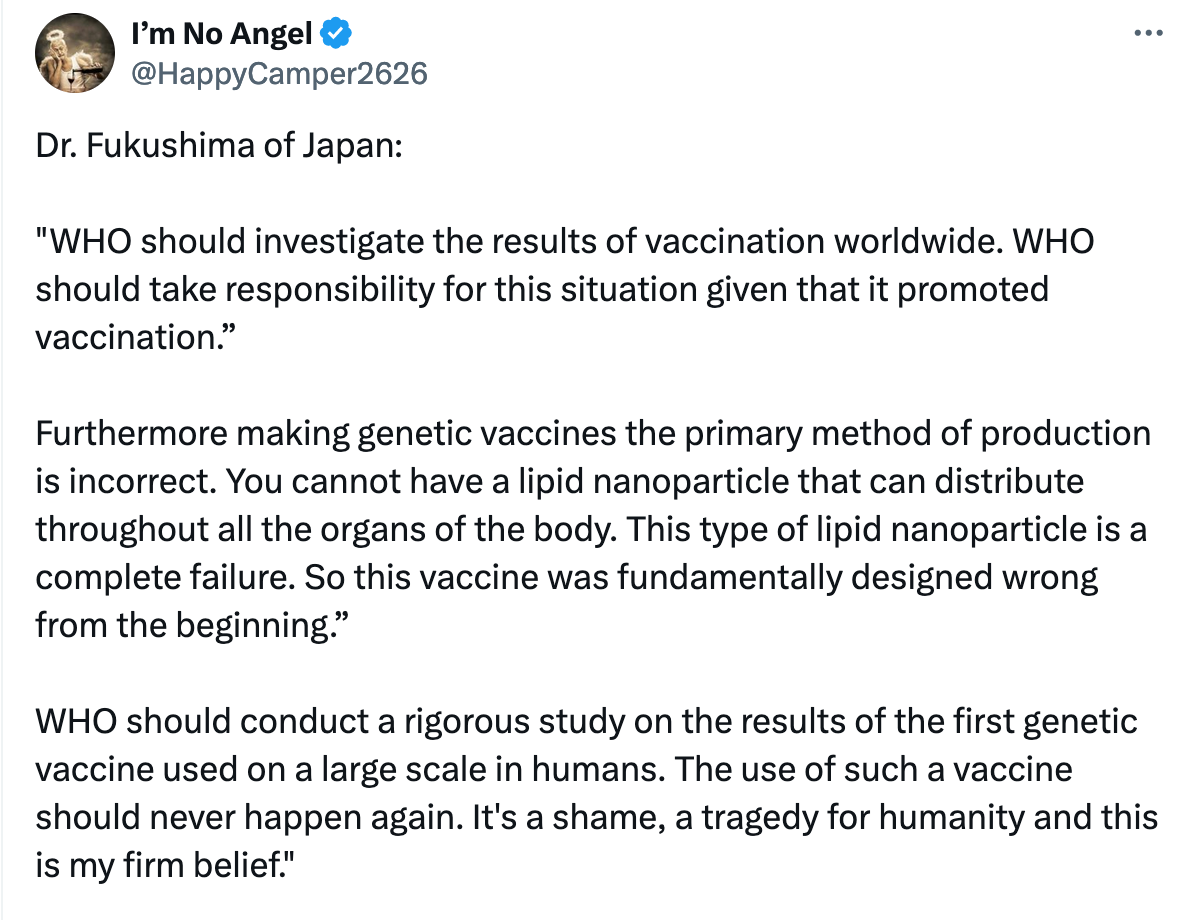
But the statement about “all over the world” is also quite misleading.
For example, Japan actually reported to VAERS that the vaccine was indeed responsible for some deaths.
Analyzing Japan VAERS death reports

Key takeaways: Japan is probably the only country where healthcare professionals are willing to go on record in the VAERS writeup that a death was actually related to the mRNA vaccine There are three levels of certainty within the reports - related, probably related and possibly related
And some prominent scientists from Japan have already called for the mRNA technology to be banned.
And we recently learnt that the Japanese health agencies removed the question which asked if the patient was vaccinated, when Doctors were filing death reports5.

Is Japan not considered part of the world anymore?
How many people had a serious adverse reaction?
Let us now move on to the next response by Dan.
@00:04:03: So let's listen to them.
Del Bigtree: Of the 10 million people in this system, 782,913 checked this box. They checked the box. I went to a doctor.
Dan Wilson: So in that segment of the talk show, they're talking about a previous lawsuit as if they revealed any new information when this information was already public. So let's look at the actual published research and see if it matches what he just said. And would you look at that? No, it doesn't really match that. Of all the participants who responded to VSafe, about 9.7% said that they were unable to do normal activity following their first dose, and 26.5% said that they were unable to do normal activity after their second dose. This doesn't sound unusual. After my third dose, I felt like crap. I had aches and I just felt really crummy. But the next day I felt fine. It's normal to feel like that during an immune response, your immune response gives you aches and pains and possibly fevers and headaches and things like that.
@00:05:01: But the numbers who said they actually reported seeking medical care are much smaller. That was around 0.8% after the first dose and around 0.9% after the second dose. And medical care might just mean taking Tylenol or going to the pharmacy to pick up something to deal with your symptoms. Even smaller numbers reported seeking a telehealth consultation. Even smaller numbers reported visiting the clinic for their symptoms. And even smaller numbers than that reported going to the emergency room or actually being hospitalized because of whatever symptoms they were feeling. So when the research is done properly using this data and statistics are applied, let's see what the authors of this paper actually say about it. They say that reports about the measures of health impacts used in v safe, although self assessed and subjective, correlate with reports about reactogenicity.
First of all, if 1% of the participants require medical care, that is not a good thing. This is another example of a third rate safety standard. This means if you vaccinate 100 million people, this means nearly a million people will need medical care.
And of course Dan anticipates this objection, and says “And medical care might just mean taking Tylenol or going to the pharmacy to pick up something to deal with your symptoms“
You know how we can find out for sure?
By reading those free text entries which the CDC refused to publish!
Now, I do agree with the bigger point Dan Wilson is making here. 7% of the v-safe participants did not require medical treatment for a serious condition. It is probably closer to 1% or less than that. It is hard to be sure what Del Bigtree is actually claiming in the video clip.
However, the real issue is that we had no way to confirm any of the numbers published in the v-safe papers until the CDC made all this information public.
And even though Dan dismissed this is as old information, CDC only published even the aggregate numbers (which Aaron and Del show on the dashboard) after being sued, and they released it only in 2023, after approving the COVID19 vaccine for children.
In a future article, I will explain why the free text entries are necessary to verify even these aggregate numbers6.
Skillset deficit
I have already mentioned how there seems to be major skillset deficits among the vaccine pushers.
The "Grand Debunk" is wrong about VAERS

Summary The “Grand Debunk” of the “Turtles” book on the Science Based Medicine (SBM) website is written by people who seem to lack basic data science skills v-safe free text information was not actively monitored, and you will know this if you had basic knowledge of Natural Language Processing
Do you think that also affected v-safe data analysis?
Dan says this in the video
So again, they're using VSafe in conjunction with other safety monitoring systems and seeing if they agree with each other.
@00:06:05: This is what scientists do. They ask a question and then attack it from multiple angles to see if the evidence yielded from multiple angles are all consistent with each other. And in this case, they didn't find evidence of anything that was overtly concerning. In other words, they didn't find anything that was causing mass suffering or mass death that would be unexpected following a mass vaccination rollout.
First of all, the evidence from Japan is already inconsistent with what the rest of the world is reporting, as I mentioned before.
But these vaccine safety researchers don’t even know what question to ask.
For example, how could anyone with even rudimentary knowledge of Natural Language Processing allow CDC to publish its v-safe paper?
CDC's v-safe text mining is laughable

This is Part 6 of my Case for Vaccine Data Science series. I was reading a paper about CDC’s v-safe free-text-response analysis, and it is just laughable. First, remember that all the “solicited” responses were just check-the-box fields for known, benign vaccination side-effects and any other adverse reaction was only captured by the free text responses …
Do the paper reviewers even know it is possible to use an NLP library like spaCy to do this free text analysis? Why would anyone still be using string regular expressions in the 2020s?
To me, it looks like there is a structural “NLP skillset deficit” among the vaccine safety researchers who review and write these papers.
Given that they failed to do even basic verification of CDC claims, to suggest these scientists were “attacking” this question from “multiple angles” (which makes it sound as if they were leaving no stone unturned) seems completely absurd.
The importance of data science
As you can see, my Substack is called Vaccine Data Science.
The field of data science is based on the premise that we can identify important patterns in large datasets by writing some code, looking at the results, and iteratively improving our code to get better and better answers. This is almost the exact opposite of the sentence that Dan says below (in emphasis).
Aaron Siri: Yeah, they were withholding the free text fields. Those are fields in which individuals using the v safe system, those 10 million individuals, could write in whatever they wanted. And the reason that those free text fields and the data in those free text fields are so critical.
Dan Wilson: So that's just him explaining the free text fields that I mentioned earlier. That was the whole point of this current lawsuit. And he doesn't explain what they expect to learn from it or why they are so important, because really they're not. Unless you do some epidemiological statistics on them, which you're probably not going to be able to do with that kind of data, you're not going to learn anything.
@00:07:04: But what he says next is just fantastic.
First of all, I do think Dan Wilson is being sincere when he says this.
But I also think that approach is problematic.
I will explain why using an anecdote.
The main reason I first started investigating VAERS around August-September 2022 was this:
a) a lot of people7 were claiming on Twitter that anyone can file a VAERS report, and they would post a screenshot of the Incredible Hulk VAERS report
b) I would go to OpenVAERS and read a list of the most recent reports and notice that they all seemed genuine. I would go through many tens of such reports without encountering a single “prank report”.
So this raised a question - is it even possible to quantify how many reports could be prank reports8?
That led to this initial investigation, which I then consolidated into a larger article:
Quantifying "crazy" VAERS reports

One of my first articles talked about how you can calculate a Machine Learning based “medical jargon” score for the narrative text using spaCy’s biomedical NER models. I refer to this medical jargon score as ENTITY_SCORE in the rest of this article. In my view, you can use this score as a proxy for checking if it is a fake/prank report.
My estimate is that prank reports are less than 1% of all reports and thus can be safely ignored9.
The first reason I proceeded with my analysis was because I did not have to submit a proposal for doing this work (this is why VAERS, despite its many flaws, is such an amazing dataset). Second, I did not know beforehand how exactly I was going to estimate the percentage or whether I would even be successful, and tried different things along the way. Third, I was not interested in an exact percentage of prank reports. I just wanted an estimate, because I could proceed to do further analysis confident that prank reports will not have a major impact on my analysis.
I should also point this out - the field of data science is usually more interested in finding patterns than in generating complete datasets10. For example, it is possible that more than 1% of reports are prank reports. It is also possible less than 0.1% are prank reports11. But the number is still a very small percentage.
Why does this anecdote matter?
If I had to fill out a form to get approval for this analysis without having any idea of what I might find, then I probably wouldn’t have even bothered with the analysis in the first place.
In other words, explaining “what you expect to learn from it and why it is so important” is an excellent way to ensure you never do this kind of exploratory research12.
Adverse Events of Special Interest
This topic is where Dan Wilson seems to be lacking a basic understanding of what actually happened with v-safe data analysis.
He says
Dan Wilson: I don't know why anti vaxxers cannot get this right. Adverse events of special interest are not adverse events that are known to be associated with whatever medication or vaccine is being rolled out. Adverse events of special interests are predetermined. Adverse events that are required to be reported following the administration of any medication or vaccine, they are predetermined.
@00:08:01: Let me give you an example. If I'm running a clinical trial and I want to submit a list of all adverse events that I want immediately reported after the administration of whatever I'm studying, I submit an adverse events of special interests list. So before the drug or intervention goes into anybody at all, I have to submit a list that is usually as broad as possible of any adverse events that could follow the intervention. And these adverse events, again, don't have to be causal. One of the AESis for Covid vaccines was Covid itself. Obviously, Covid vaccines do not cause Covid. But if we want to know how frequent a COVID infection is after administering a vaccine, that would be important to know. When analyzing data in no way, shape, or form does a list of ASI's imply that researchers knew that those events would happen because of the vaccine. This is now a very old anti vaccine trope that just won't seem to die. And I'm not sure why anti vaxxers can't seem to learn why they're wrong about this.
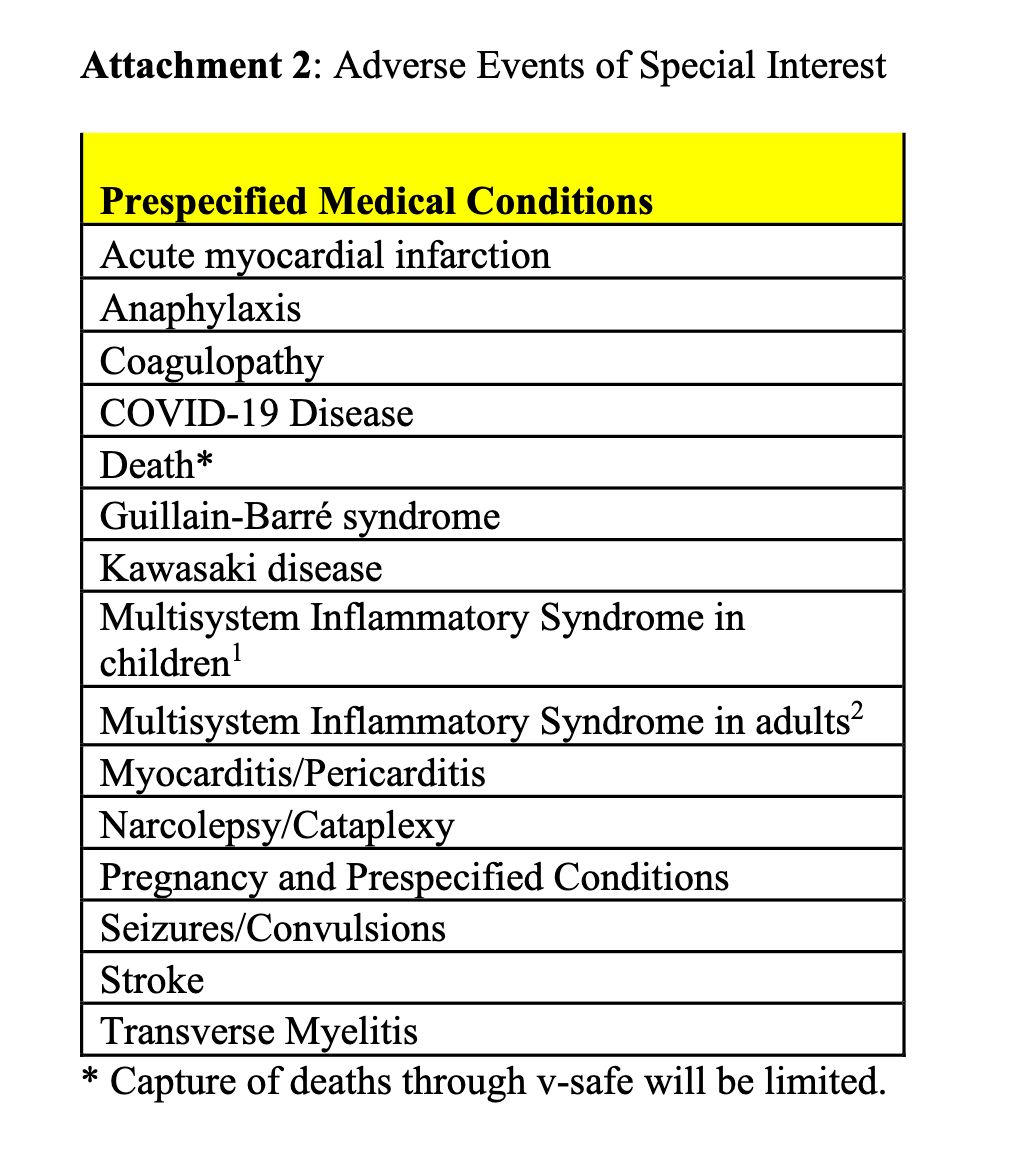
But this is directly contradicted by the CDC’s own v-safe protocol document where they explicitly mention that the Adverse Events of Special Interest will be monitored using a pretty elaborate process:
For v-safe participants who have a VAERS report submitted through the VAERS call center, additional analyses will be conducted. Rates of serious events as well as adverse events of special interest (AESI) following COVID-19 vaccination will be generated using VAERS reports solicited via v-safe to define the numerator and v-safe participants as the denominator (Attachment 2). VAERS reports that are considered serious or AESI will be reviewed by medical staff at CDC. Case definitions (Brighton Collaboration or other standard definitions as appropriate) will be applied to the AESIs. Reporting rates for each AESI will be calculated and compared to established background rates. If at any time rates observed in v-safe exceed what is expected from background rates, further investigation will occur within other vaccine safety monitoring systems, including VAERS and Vaccine Safety Datalink (7).
Note that Attachment 2 only had about 15 adverse events. This is not a broad list of any and all possible adverse events, but rather a pre-selected, pruned down list of adverse reactions based on some previous analysis done by the Pharma companies.
And from all indications, it looks like the CDC did not do what they promised in their Analysis Plan.
A transparent analysis would have involved the following:
describing the keyword search algorithm for identifying the 15 AESIs from the free text entries
explaining the decision tree used to decide whether or not the AE was related to vaccination
publishing the raw counts for the initial keyword search and the actual count of AEs considered to be related to the vaccine (for each AESI)
releasing the anonymized free text entries so the public can verify that the CDC did follow their own protocol
Since none of these AESI’s were included in the check-the-box list, the only way to do these calculations is to write some code which can search for these symptoms in the free text entries.
How rare were the AESIs?
The vaccine pushers face an inherent contradiction if the AESIs are truly rare, as they claim.
If an AESI is truly rare, unsophisticated “keyword search” will never yield enough search results (in the free text entries) to exceed background rates. In other words, it is a simple way to test and discard the possibility that your AESI is occurring at higher than expected rates.
And why is that?
That is because a simple keyword search for AESIs will provide very high accuracy compared to statistical Machine Learning algorithms. On top of that, if the AESI is also very rare, then it should be possible to read the entries corresponding to the search results manually and report the raw numbers. Why didn’t the CDC do it? One objection could be that this could miss some reports if the keyword was chosen incorrectly, or if there was a typo. But the number will still establish a floor for the total number of AESI reports, and could still be used to calculate the background rate as long as the CDC was transparent that this is how they did the calculation.
If this raw number exceeded the expected background rate, it should have prompted further investigation. If the number was less than background rate, the CDC could have simply mentioned in the Limitations section that a simple keyword search strategy might not uncover all the cases, and further analysis would be necessary to be certain13.
But the CDC did NOT publish such an analysis for these 15 AESIs.This begs the question - even if the CDC had the best of intentions (for refusing to publish the analysis) AND did the analysis behind the scenes without making a single mistake, how can anyone claim these are the most “well studied” vaccines in history?
No independent entity has even done a proper audit of the free text entries well into 2024!
In fact only one CDC paper even published sample free text responses, so we did not even know what these free text responses looked like till the recent FOIA release which began in 2024.
Are v-safe free text entries just as “crazy” as VAERS?
The next section in the video is a great example of Dan Wilson’s overall dim view of self-reported adverse reactions.
Del Bigtree: Look, I don't want to make light of it, because I know we're about to start reading some really horrific stories. And I remember when we were talking about this, CDC was pushing back. They were trying to say things like, well, you shouldn't have to. You can't read all of those fields. We're going to categorize them. We'll just categorize them and give them a code and put the different things. And they didn't want to let us read the writing.
Dan Wilson: Yeah, it's almost like they just don't want you misrepresenting data again. People could have written whatever they want in these fields. It could have been a complete lie. It could have been not related to the vaccine. It could just be something that they think is related to the vaccine, but really it wasn't. If you want to be scientific about it, you have to have a way of determining whether or not what you're reading is actually significant or reflective of a real experience that is going to affect the rest of the population in any meaningful way.
@00:10:03: That's why scientists do epidemiology and statistics. With these data, we don't just read one experience and say, oh my gosh, look at this. This must mean something. Delbigtree and Aaron Siri don't care about evidence. They just want to get an emotional response out of their viewers so that they keep giving them money. That's what all this is about, what.
In other words, Dan probably thinks that v-safe free text entries could also have a lot of prank reports like VAERS does.
There is a big problem with this assumption.
Most of the v-safe entries span multiple days and many of them span multiple weeks and months14. In other words, there were actually a lot of AESIs which happened to people whose first check-in indicated that they had no problems whatsoever. If the v-safe participant wanted to play a prank, why would they go to all that trouble to send in a “Everything is OK” check-in as their first one? It doesn’t really make much sense does it?
While I do agree with the other possibilities (the adverse reaction may not have been related to the vaccine), that is not a good reason for the CDC to refuse to publish it.
The main advantage of v-safe: Active surveillance
Dan is right about this next section:
Del Bigtree: The judge is saying. Are you telling me that the CDC has all this data and the only thing you've looked at is the first two weeks when the entire question with an emergency use authorization is, what about the long term side effects? What about two years down the road? What about six months? What about all these issues of blood clotting we're seeing? And they only look two weeks? This judge, I mean, anybody with blood moving their brain would have to be saying, oh my God, this is insane.
Dan Wilson: Oh my God, this, this is insane. That's a classic del big tree rant for you. So if you look at the VSafe data, the greatest number of reported events occurred on day one following the dose of vaccine being given.
@00:11:01: From there, the average number of reported events declines each day. So even if they're just looking at the first seven days, you're capturing most of the reactogenicity that is happening with these vaccines. But again, VSafe is not the only database we use to assess vaccine safety. It's there to supplement the many other vaccine safety reporting databases that we use.
But this doesn’t address the objection raised by the Judge!
If you have an app like v-safe which is actually capable of long term surveillance, why would you restrict yourself to a 14 day analysis?
But there is also a second and much more important reason to extend the data analysis window to be as long as possible.
If there are potential long term side effects which are related to the vaccine, it should be easier to investigate what happened if the user has already done a lot of check-ins using an app like v-safe, compared to someone who goes to the Doctor only on the date of symptom onset. In fact, I believe that is one of the main reasons v-safe is considered to be “active surveillance”?
So why wouldn’t you extend v-safe studies to longer time windows?
Conclusion
The only “scam” here is that this lawsuit and the v-safe free text data isn’t getting more attention.
And I found it to be very useful for doing and presenting research, even if I say so myself.
To put it in context, Pfizer’s revenues jumped from $40B in 2020 to $80B in 2021, and then to $100B in 2022. Imagine doubling your revenue from a base of 40 BILLION in a single year. But of course, it is all supposed to be fine when Pharma companies do it! :-)
I only consider the interesting/relevant transcript sections, so I recommend reading the full transcript at least once in case you feel like some context might be missing
This doesn’t automatically mean there is a cover up. One of the biggest things I learnt during the pandemic is that there are often very benign reasons for what looks like malicious behavior. But my overall point still stands - a lot of the data we can use for verifying the COVID19 vaccine’s safety is not being published, and sometimes not even being collected.
In fact, I am now quite certain that without doing a proper analysis of the free text entries, it isn’t even possible to fully make sense of the v-safe data.
No doubt some of them were true believers, but now I think a fair number of them were probably Pharma bots
And of course, once I figured out how to do my first analysis, it didn’t take me very long to notice that no one was doing any serious analysis of the text writeups in VAERS. So I just kept going, and I have now published nearly 100 articles on just the topic of VAERS text analysis! And something tells me that my prolific output is not a function of my dazzling brilliance :-) I think it is more a function of how almost no one with the appropriate skill set is analyzing vaccine injury datasets :-(
In the sense that they don’t add any useful signal to overall VAERS analysis
Funnily enough I have seen
ask why this or that data is missing from my VAERS analysis. The answer is pretty simple: the goal of data science is not to produce complete or real time datasets, but to identify trends and patterns.For example, I used a pretty stringent value of 10+ for my EntityScore. If I reduced it to 5+, the number of “possibly” fake reports would go down quite a bit.
And the speed of each iteration also matters. If it took me days and days to run one experiment, then I would also favor the prepared approach Dan suggests. But that’s not really necessary nowadays. Using my MacBook I can load the entire 25GB v-safe dataset (~150 million records) into DataGrip and run SQL queries and get answers within minutes.
In case you think my suggestion doesn’t make sense because it would have attracted more scrutiny, you should know that the CDC has already published a paper which said almost exactly that!
Menstrual irregularities and vaginal bleeding after COVID-19 vaccination are being reported, although this study is unable to assess whether these events are caused by COVID-19 vaccination. Text analytic methods can speed up the identification of potential vaccine reactions that are not prespecified in structured data collection. Further studies are needed to better understand their prevalence and pathophysiology.
This is in stark contrast to VAERS, which collects all the information in one web session. To the best of my knowledge, there isn’t even a way to “save" your work and come back to it later when you use the online VAERS report form.
I think data science is to get the most insight with the least amount of work to find patterns..., so peabodies can stay in the "hypothesis" zone... You never said anything about the ~170K adolescents in vsafe? Del & Aaron even missed it or haven't said anything about that factoid. Have you seen it yet?
I am grateful for what you do. Thank you for this analysis.