

v-safe death reports are a good example of third rate pharmacovigilance
It is also an example of an end-to-end failure of the public peer review process

Summary:
The CDC coded over 1,700 v-safe registrants with the MedDRA code "Death," but failed to mention deaths in their seminal June 2022 Lancet paper about vaccine safety.
According to the DATE_CODED field in the MedDRA CSV files, the CDC didn't even begin coding symptoms in v-safe until October 2022. If true, it is an admission that CDC did not investigate the v-safe death reports prior to approving the COVID19 vaccine for children.
Dan “Debunk the funk” Wilson presented the v-safe data in a video emphasizing declining rates of adverse events as severity increased, but missed discussing death reports and made incorrect claims about v-safe capturing most reactogenicity in the first seven days
For example, using a 42-day risk window instead of the 7-day window presented in the Lancet paper would increase adverse event rates approximately five-fold for the severe outcomes
The medical community often lacks the technical skills needed to analyze large datasets like v-safe, which contains about 140 million rows of data that even standard data science tools like pandas struggle to process
Poor coding practices by the CDC, such as marking entries like "I almost died from pain" with the MedDRA code "Death," undermine the quality of pharmacovigilance data
The rise of vaccine skepticism and so-called "grifters" who exploit it, stems at least partly from inadequate pharmacovigilance by the medical establishment
A few weeks back
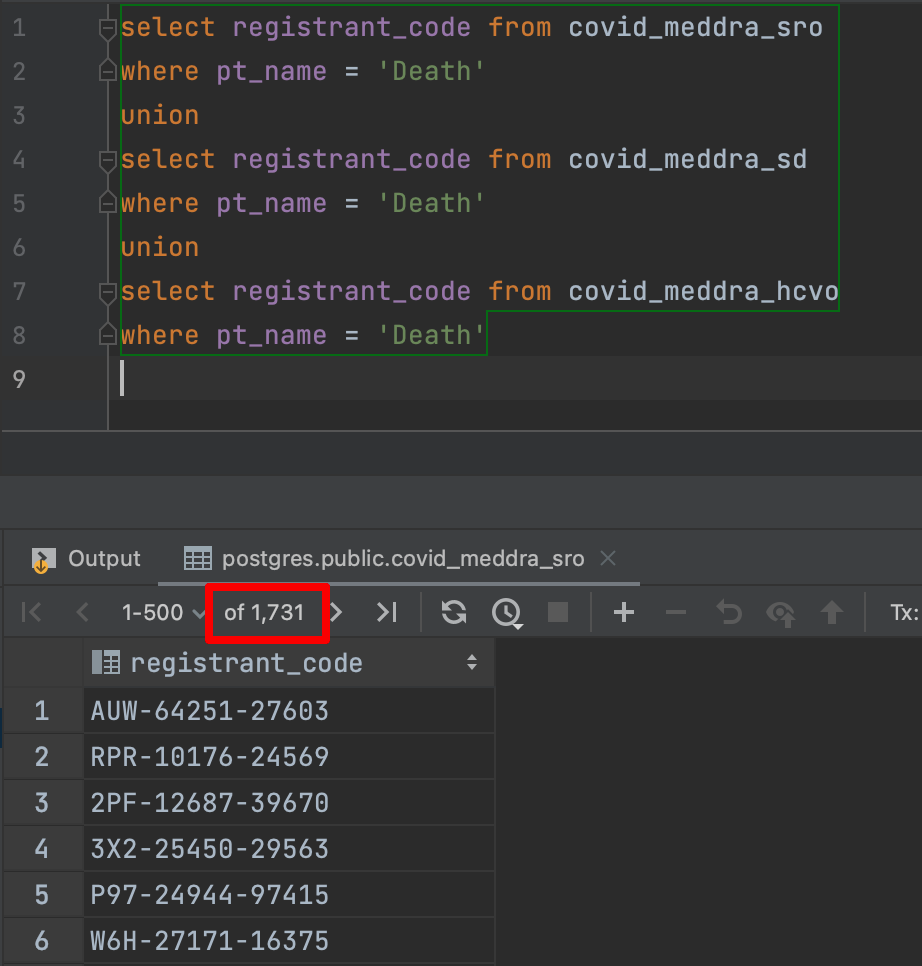
pointed out that there were now over 2K deaths1 in v-safe. Given that v-safe does not really have a way to report death using check-the-box options, it was already a bit of a surprise.And then I saw that the CDC had already coded that over 1700 v-safe registrants with the MedDRA code “Death” in the three MedDRA files.
The reason this is surprising is that there was no mention of deaths reported from v-safe in the seminal v-safe paper published by the CDC
Why I use the June 2022 v-safe Lancet paper as my primary reference
In the rest of this article, I will be using the June 2022 Lancet paper published by the CDC as the primary reference.

First, it is the most cited paper about v-safe according to Google Scholar
Second, it was cited in a video by Dan “Debunk the Funk” Wilson as an example to show how safe the mRNA vaccines were.
Third, this is a good followup to the article I published about how the CDC ignored all the free text information in their September 2021 paper.

The CDC did not even “code” the “Death” free text entries until November 2022
All the MedDRA codes CSV files - covid_meddra_sro (systemic reactions), covid_meddra_sd (symptoms description) and covid_meddra_hcvo (healthcare visits) have a column called DATE_CODED.
At first I did not understand why the CDC was so keen to publish this column in the CSV file.
Especially given that they did not bother to publish a date column where it would have actually been more helpful - in the freetext tables (to be more precise, they should have added the RESPONSE_ID column, which would have allowed v-safe researchers to infer the date). As a result the CDC has made the free text entries far less helpful than they could be. So I looked at the earliest date when Death was coded as a symptom. It was November 2022.

And what about the earliest date_coded for ANY symptom? It was only in October 2022, so not much earlier.

Why did the CDC start coding the symptoms only in October 2022, often a full year after the free text data was submitted by the majority of v-safe registrants, and well after the COVID19 vaccines were approved for children?
Even if it was unintentional, it is still third rate pharmacovigilance.
The CDC did not mention Death as a potential adverse event within v-safe in their Lancet paper
In the Lancet paper, you will see the following table (Table 5). The calculation is based only on check-the-box symptoms.

Notice that Hospitalization is less than 0.1% and thus very rare2.
And Dan Wilson walks people through the list, explaining how the percentages get lower and lower as you go all the way down to the end of the table (emphasis mine):
@00:05:01: But the numbers who said they actually reported seeking medical care are much smaller. That was around 0.8% after the first dose and around 0.9% after the second dose. And medical care might just mean taking Tylenol or going to the pharmacy to pick up something to deal with your symptoms. Even smaller numbers reported seeking a telehealth consultation. Even smaller numbers reported visiting the clinic for their symptoms. And even smaller numbers than that reported going to the emergency room or actually being hospitalized because of whatever symptoms they were feeling. So when the research is done properly using this data and statistics are applied, let's see what the authors of this paper actually say about it.
In case you did not notice, the table stops at hospitalization without mentioning deaths3 at all, even though people with common sense usually want to know the answer to that question and would like to see that information provided at the end of the table.
I am not suggesting Dan Wilson thinks there were no deaths reported in the v-safe data.
But I am suggesting that the fact he does not mention it (if only to point out that the numbers would be even lower) gives the casual video viewer the impression that there were no deaths at all.
Why didn’t the CDC make the effort to add it into the paper?
Another example of third rate pharmacovigilance.
Ironically, in the very next minute Dan Wilson claims this:
@00:06:05: This is what scientists do. They ask a question and then attack it from multiple angles to see if the evidence yielded from multiple angles are all consistent with each other. And in this case, they didn't find evidence of anything that was overtly concerning. In other words, they didn't find anything that was causing mass suffering or mass death that would be unexpected following a mass vaccination rollout.
Looks like Dan himself fell far short of the lofty expectations he sets for his peers in the medical community. But Dan shouldn’t feel bad, since he is certainly no worse than his peers, who did not raise the question either.
Someone might object - the information provided in the table is based on check the box symptoms which are amenable to SQL query reports, while the Deaths needed to be coded first.
But you cannot have it both ways!
If the deaths were really so rare then the CDC had plenty of time to have someone look into the free text and find them and publish all the relevant stats in their paper.
If not, then there was some cause for alarm and the CDC’s first job was to get to the bottom of the issue (by issue, I mean free text entries which have words like “died” and “passed away” etc) and not publish anything until the matter was fully resolved.
Another example of third rate pharmacovigilance.
The typical 42 day risk window would have increased the published AE rates
Suppose you do think that less than 0.1% hospitalization rate is not all that bad given that COVID19 was such a dangerous4 disease.
But the rates provided in the table is only for the first 7 days.
Using just the check the box symptoms, you will find that the rate increases about 5X for all the outcomes if you use a risk window of 42 days.
You might be wondering - is there anything special about 42 days?
First of all, there is already plenty of literature discussing the importance of a 42 day risk window.
Second, v-safe itself was designed to do weekly checkins until 42 days.

If your app has already been designed to collect information for up to 42 days, why wouldn’t you do an analysis based on that risk window?
Dan Wilson, for example, states this from the same video shown above (emphasis mine):
Dan Wilson: Oh my God, this, this is insane. That's a classic del big tree rant for you. So if you look at the VSafe data, the greatest number of reported events occurred on day one following the dose of vaccine being given.
@00:11:01: From there, the average number of reported events declines each day. So even if they're just looking at the first seven days, you're capturing most of the reactogenicity that is happening with these vaccines. But again, VSafe is not the only database we use to assess vaccine safety.
As I have explained in my previous article, this is just provably wrong. That is, you are not capturing most of the reactogenicity in the first seven days.
Why couldn’t Dan Wilson figure this out?
The wider scientific community is not doing its job either
I am going to speculate a little bit here.
I don’t think Dan Wilson is doing this intentionally - I really think he doesn’t know how to get the v-safe data into a format which can be analyzed more easily.
For example, the v-safe checkins CSV file, which contains most of the important information, has about 140 million rows. That’s quite a lot of data. Even tools like pandas, which is used very commonly in data science, struggle to handle that amount of data. There are alternative Python libraries but the further you go down this path, the more time (and sometimes money) you need to get answers to simple questions - like what percentage of some v-safe cohort got hospitalized within the first 42 days of taking a vaccine dose?
In other words - this isn’t even a criticism of Dan Wilson. The broader medical community also lacks the skillset to do this kind of analysis.
In fact, I saw this skillset deficit so often in COVID19 vaccine safety monitoring that I wrote an entire article about it!

“But… medical professionals don’t have the time to do all this analysis!”
I think someone is almost certainly going to bring up this objection.
The basic premise here is that given enough time, Doctors whose primary job is to care for their patient, could well have studied all this and done the required analysis and eventually figured it all out. They are just short of time, and it is not their fault.
But this argument leads to some pretty bad outcomes.
As a group, medical professionals have to assume almost 100% responsibility for ensuring first rate pharmacovigilance, if they want patients to continue to trust them.
No one else is going to do it for themIf even the medical professionals do not take responsibility for ensuring first rate pharmacovigilance, then why should someone who is NOT a medical professional try and figure this all out in their spare time? And if the non-medical-professionals do spend time doing the analysis, why should they not ask for someone to fund the work? And if they ask for funds, why are people calling them “grifters”?
A natural outcome of this is that vaccine pushers only need to write a few hit pieces calling vaccine skeptics as “grifters”, and it is now enough to confuse everyone who is still sitting on the fence.
Maybe a few people are indeed grifters who are just exploiting the anti-Pharma sentiment.
In my opinion, even the rise of these so-called grifters to prominence is itself a symptom of third rate pharmacovigilance!
This would have never happened if the medical establishment had done its job properly.
Unfortunately, the CDC sometimes codes people who write in things like “I almost died from pain” as MedDRA code “Death”. Whether it is a human or some software doing it, this really poor coding system - which is yet another example of third rate pharmacovigilance in my opinion - has made it a lot easier for the vaccine pushers to make idiotic claims.
Some would argue less than 0.1% isn’t very rare if you vaccinate 300 million people, because then 300K people would get hospitalized. But let us pretend this is actually an acceptable rate for now.
I think most people will agree death is a worse outcome than hospitalization
If left untreated, which seems to have been the norm in some countries. But a Doctor in India used cheap drugs like Colchicine and got well-above-average outcomes, and he thinks that COVID19 wasn’t so dangerous if people were treated with drugs which actually worked.
https://welcometheeagle.substack.com/p/we-can-now-see-all-deaths-in-vsafe