
The problem with excess mortality studies
The problem with excess mortality studies
Only two are based on publicly available datasets, and both are spurious for different reasons

Scott Adams recently shared a video by Dr Dan “Debunk the Funk” Wilson.

The video makes the following claim - there are many studies which confirm that there was no increase in excess mortality after the COVID19 vaccine rollout.
But there is a major problem with all these studies:
Almost none of them are willing to share the data publicly.
My view on excess mortality studies
I wrote this in a previous article
My first objection is just philosophical. I don’t think vaccines should be so dangerous that they show up in aggregate mortality rate calculations.
You can read that article to understand why I also think it is nearly impossible that vaccine related deaths can be so high that they will show up in such calculations.
So I will not be surprised if Dan Wilson is correct, on this particular point1.
With that being said, let us just look at what the data says.
Data Availability
Every paper includes a “Data Availability” statement nowadays.
Let us look at the list of papers and see what the authors have to say about data availability. Dan Wilson cites 9 papers in his YouTube video’s description.
1 A safety study evaluating non-COVID-19 mortality risk following COVID-19 vaccination
“Data will be made available on request.”
2 Mortality risk after COVID-19 vaccination: A self-controlled case series study
“Data will be made available on request.”
“Data used in this study are available in NHS England’s Secure Data Environment service for England for England, but as restrictions apply are not publicly available (https://digital.nhs.uk/services/secure-data-environment-service).”
4 Safety outcomes following COVID-19 vaccination and infection in 5.1 million children in England
“The data that support the findings of this study—NIMS Database of COVID-19, mortality (Office of National Statistics), hospital admissions (Hospital Episode Statistics), SARS-CoV-2 infection data (SGSS) and primary care (QResearch)—are not publicly available because they are based on deidentified national clinical records. Due to national and organizational data privacy regulations, individual-level data such as those used for this study cannot be shared openly.“
“Data that support the findings of this study are available from the corresponding author, upon reasonable request.“
6 (This paper is not in English, so I have ignored it)
“The analyzed datasets, can be found using the following URLs: (1) the rates of excess mortality for all causes (per 100,000) associated with the COVID-19 pandemic from 2020 to 2021 were obtained from https://www.who.int/data/sets/global-excess-deaths-associated-with-COVID-19-modelled-estimates (accessed on 15 May 2023); (2) the coverage of COVID-19 vaccinations (percentage of the population that received at least one dose of any COVID-19 vaccine until 10 March 2023) was obtained from https://coronavirus.jhu.edu/vaccines/international (accessed on 15 May 2023); and (3) life expectancies at birth (2021 estimates) were retrieved from https://api.worldbank.org/v2/en/indicator/SP.DYN.LE00.IN?downloadformat=csv (accessed on 15 May 2023).”
VAERS data is already in the public domain
v-safe data was made publicly available via FOIA requests
“Data underlying the study cannot be made publicly available, as access to Danish Registry Data must be granted to researchers or institutions on an individual basis by the Danish Data Protection Agency.”
There are only two papers where the data has been published for scrutiny by independent researchers (number 7 and 8, which I have highlighted for emphasis)
But just because they don’t publish the data voluntarily2, does not mean there is a problem with the analysis. However, there are a couple of larger trends going on here, which does make me doubt the quality of the studies which refuse to share their datasets.
In case you are wondering why it matters if they volunteer that information versus someone making a request to get it. First of all, the people who are most likely to find new insights in the data are not subject matter experts when it comes to biology and medicine, and can easily be dismissed as lacking “credentials”. Second, if the authors engage in some kind of stonewalling but without outright refusing to provide the data, it would be quite challenging for outsiders to do something to get around the issue. Voluntarily publishing the datasets turns it into a permissionless system. Analysis of the worldwide cross sectional study
The worldwide cross sectional study has three major problems in my opinion
Reported vs Predicted
If excess deaths numbers are not reported by official government sources (for the respective countries), they are predicted using this methodology.
I created a dataset to see which countries were in the reported and which countries were in the predicted categories.
It has the data for both 2020 and 2021.
Filtering for a single year, there are 1703 countries in the dataset.
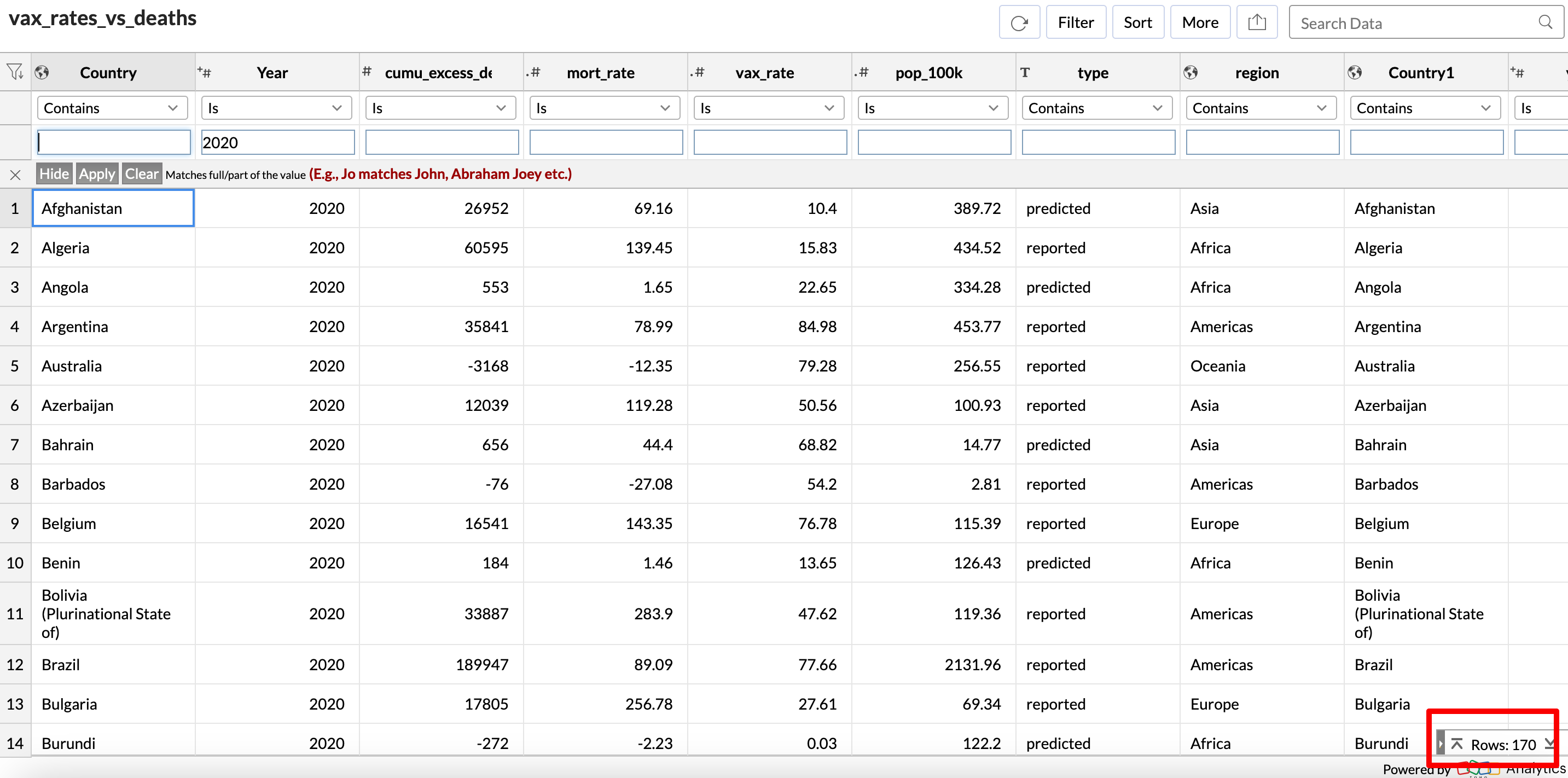
Of these, excess deaths in 69 countries are “predicted”, which is already a lot.
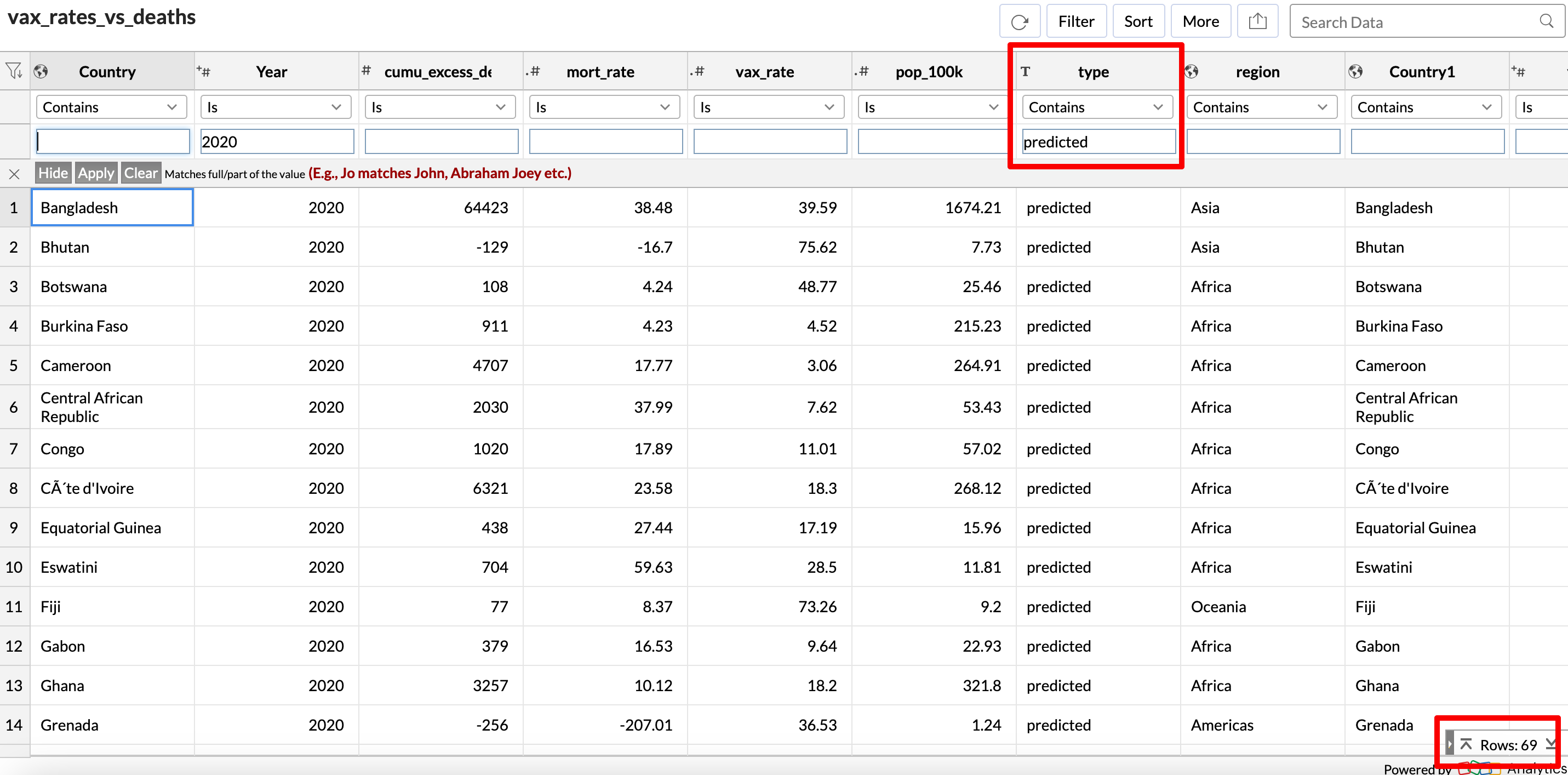
But it gets worse.
When you look at the total population of the countries where the data is reported, versus total population of the countries where the data is predicted, this is what you get:
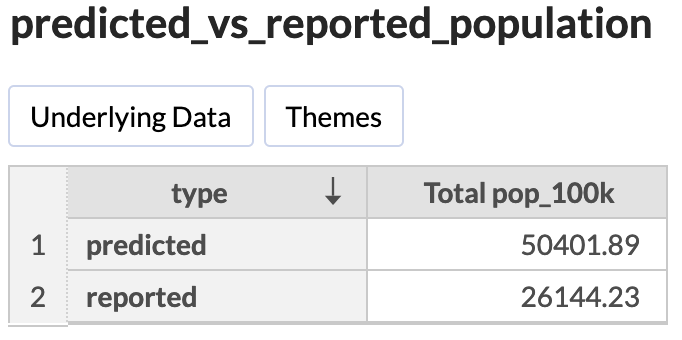
In other words, the excess deaths is “predicted” for over 5 billion people, and reported for only about half of that number.
Why didn’t the authors mention this anywhere in their paper?
2020 vs 2021
Also, the paper combines the excess death numbers for 2020 and 2021 for this map:
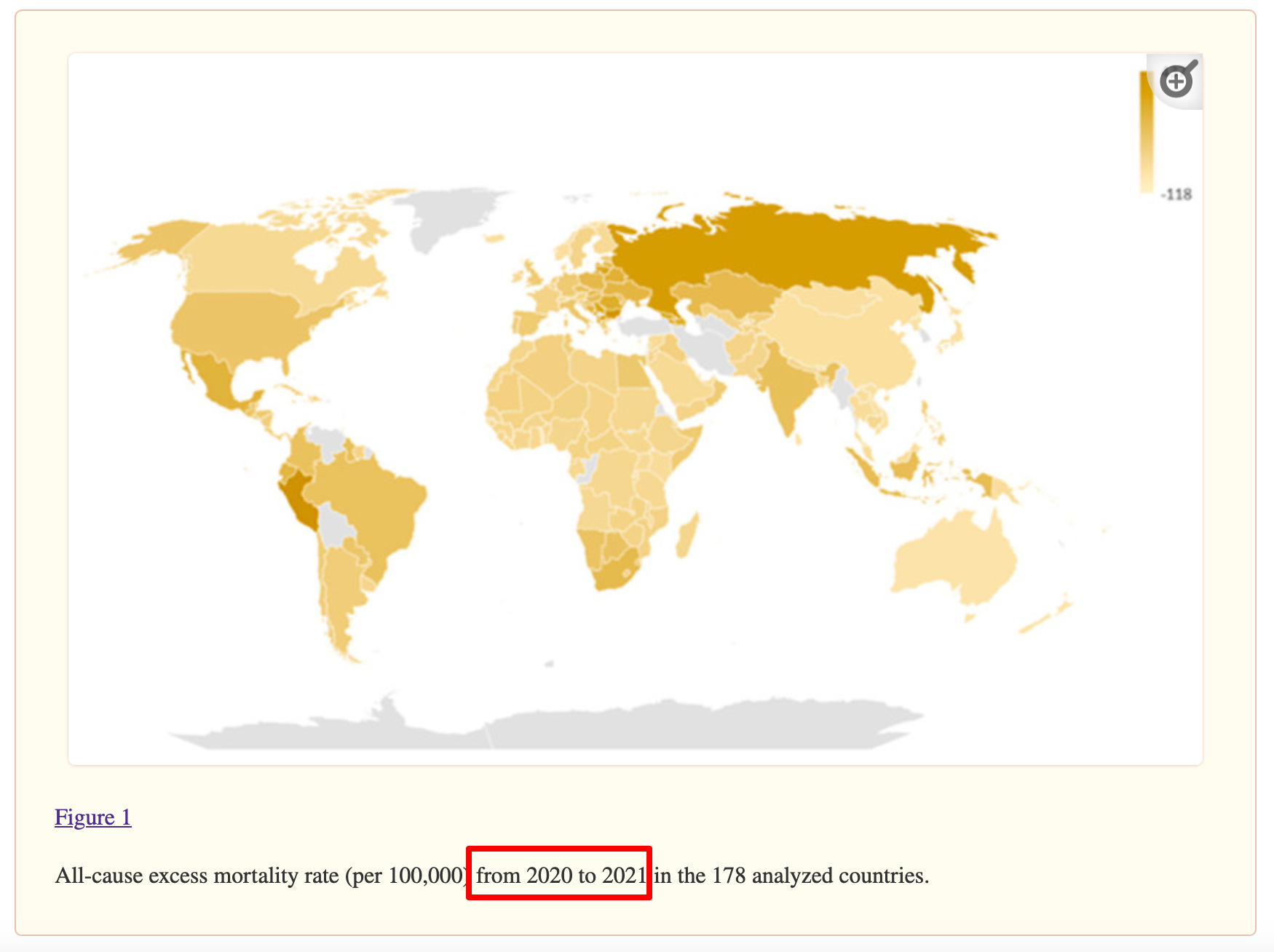
But why would you add the year 2020 into this analysis, given that the vaccines were rolled out only in January 2021?
If you plot a map for only 2021, this is what it looks like.

It even looks vaguely similar to the plot in the paper.
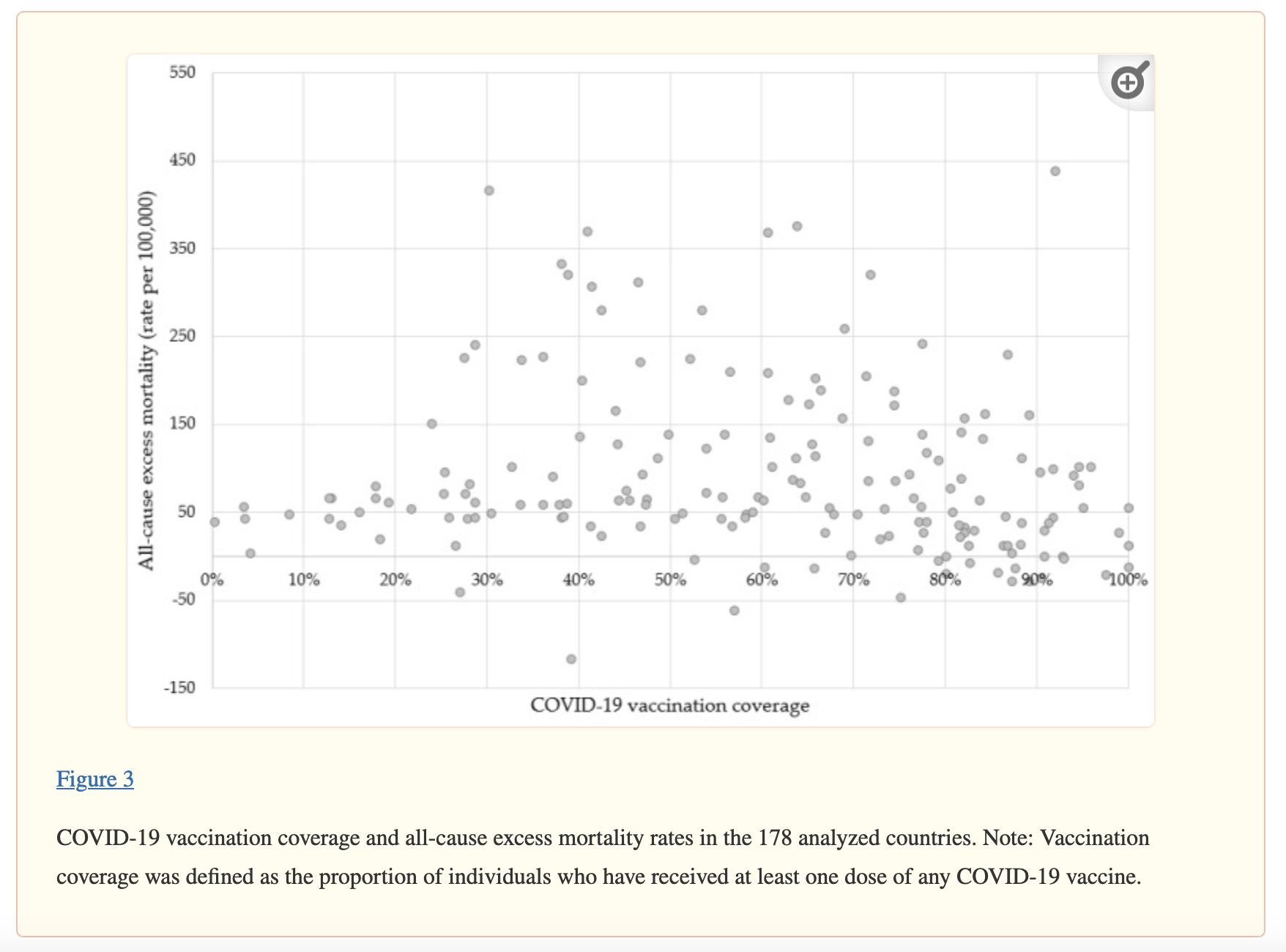
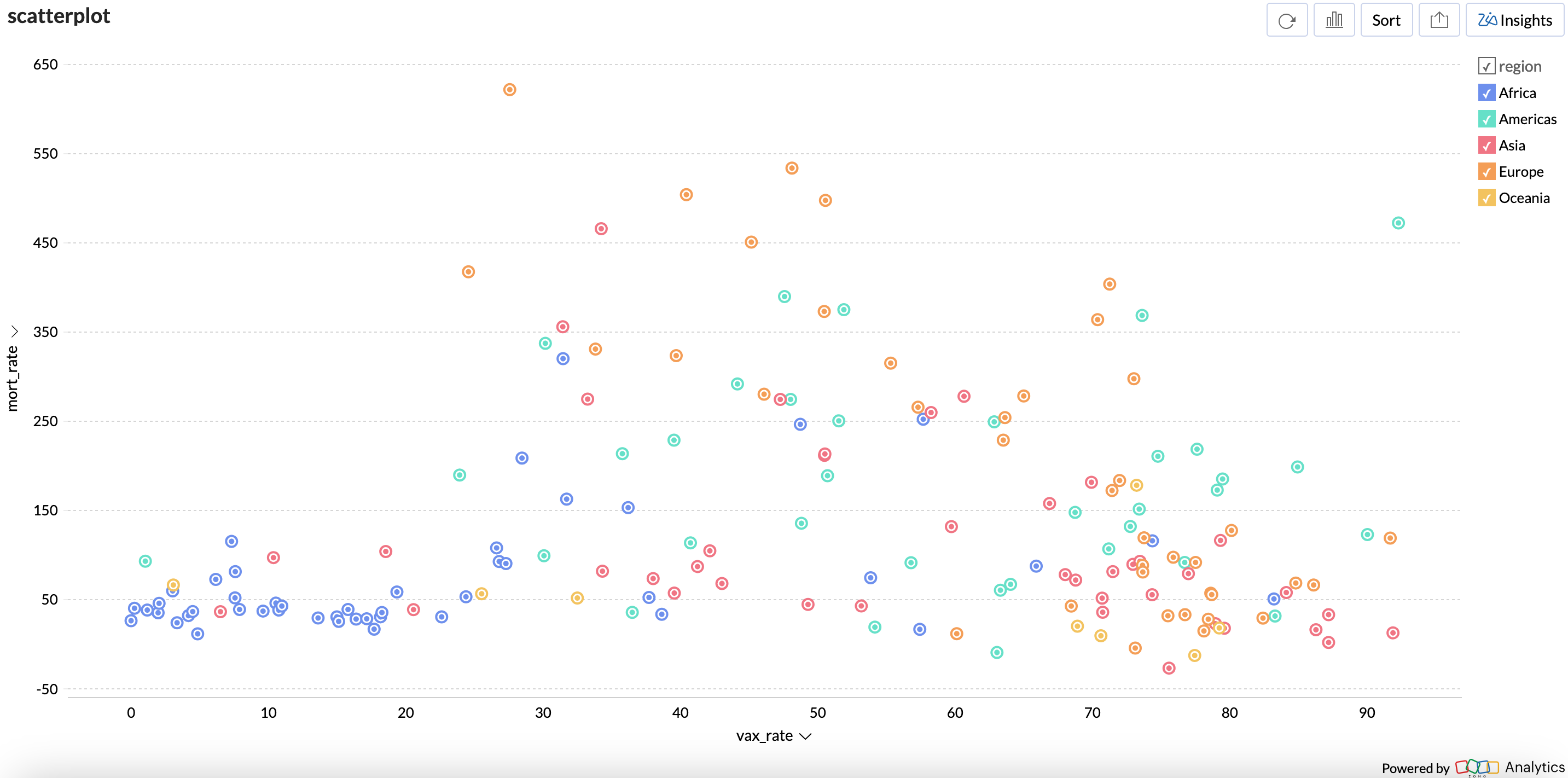
Regional differences
However, if I were to add colors representing regions, this is what the same map looks like.
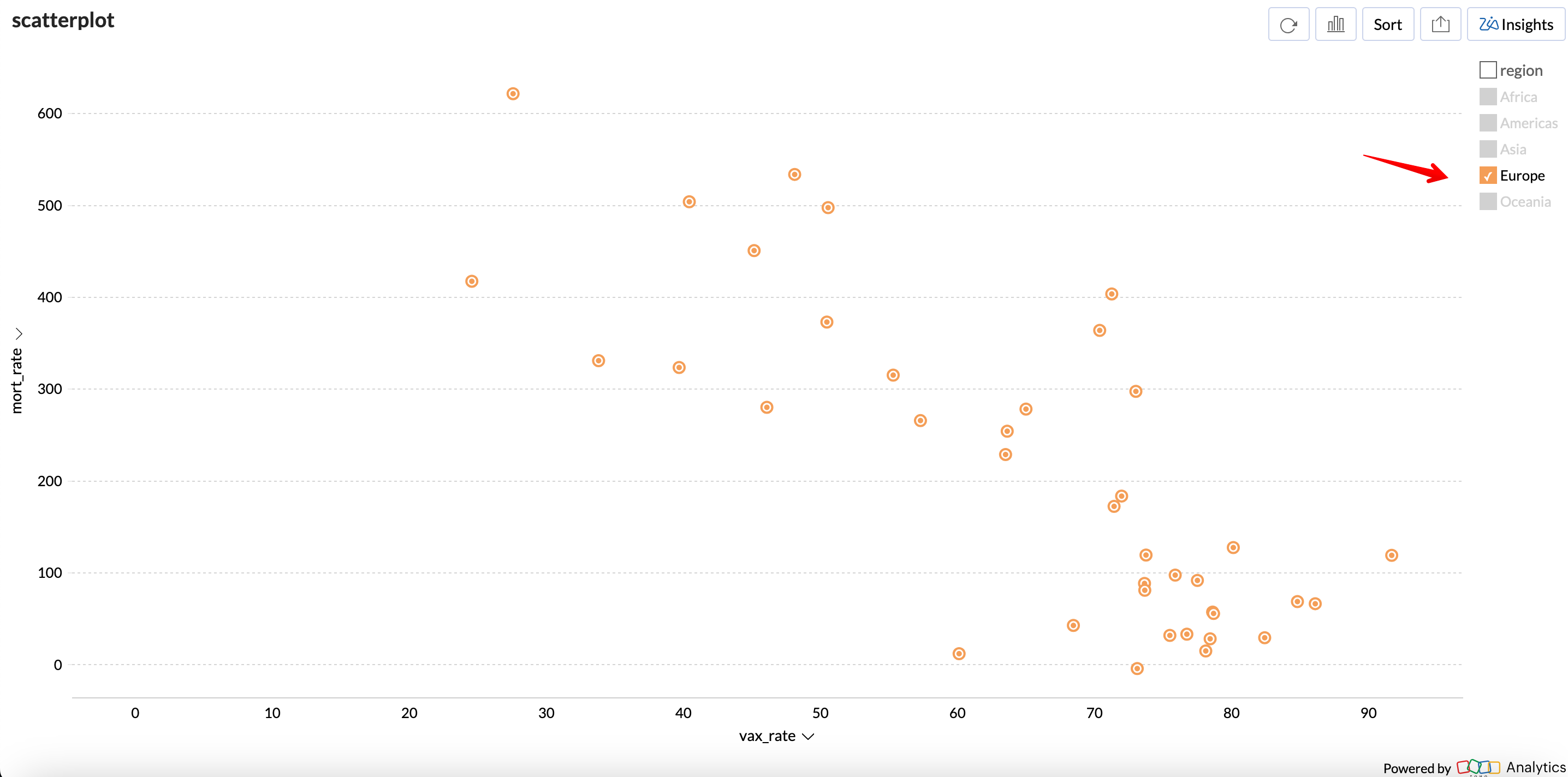
If you look at Europe, there does seem to be a negative correlation between vaccination rate and excess mortality rate.
But Africa looks quite different:
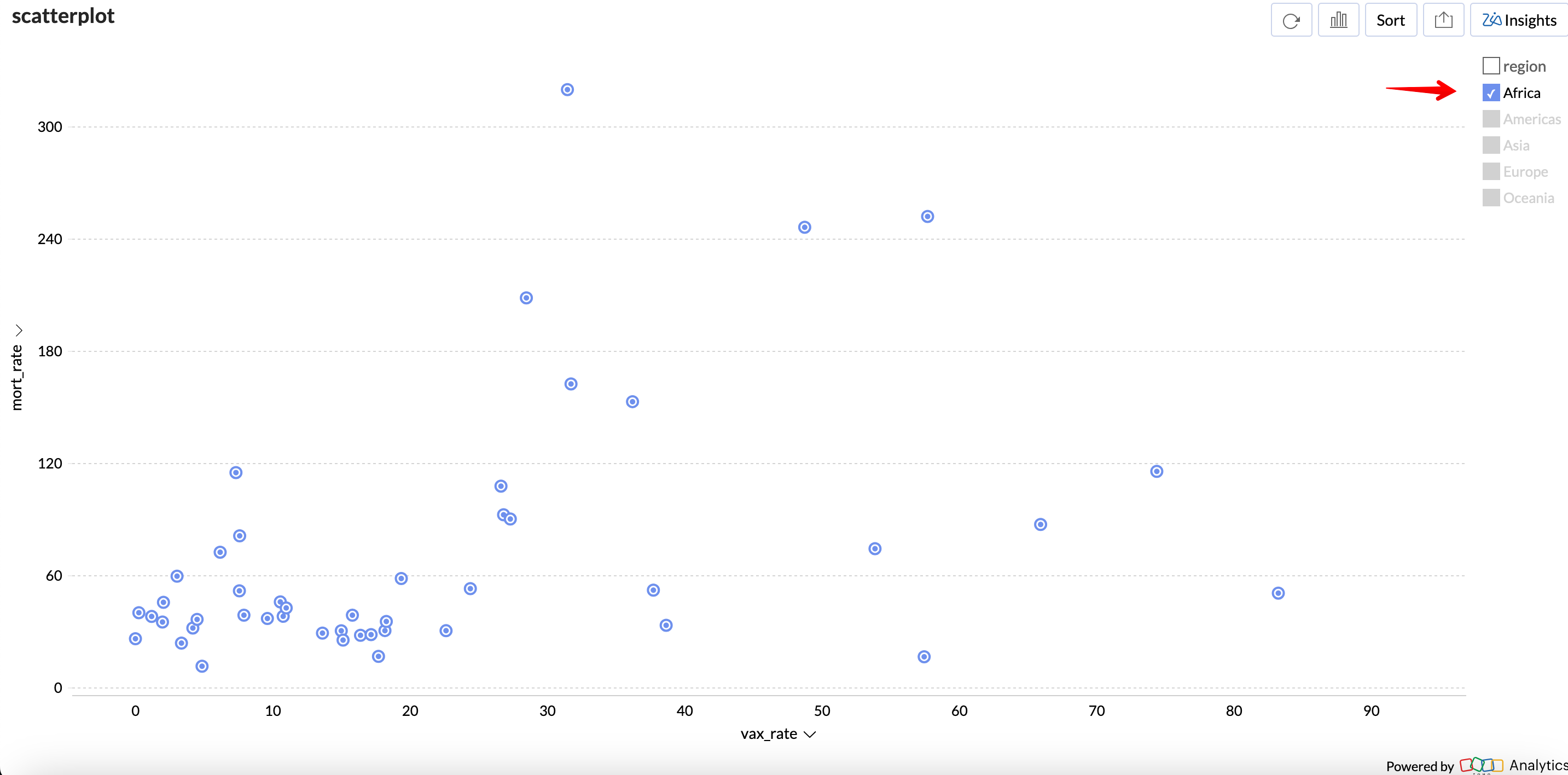
In fact, I did calculate the Spearman correlation coeffecient that they use in their paper.
There was a strong negative correlation for Europe.
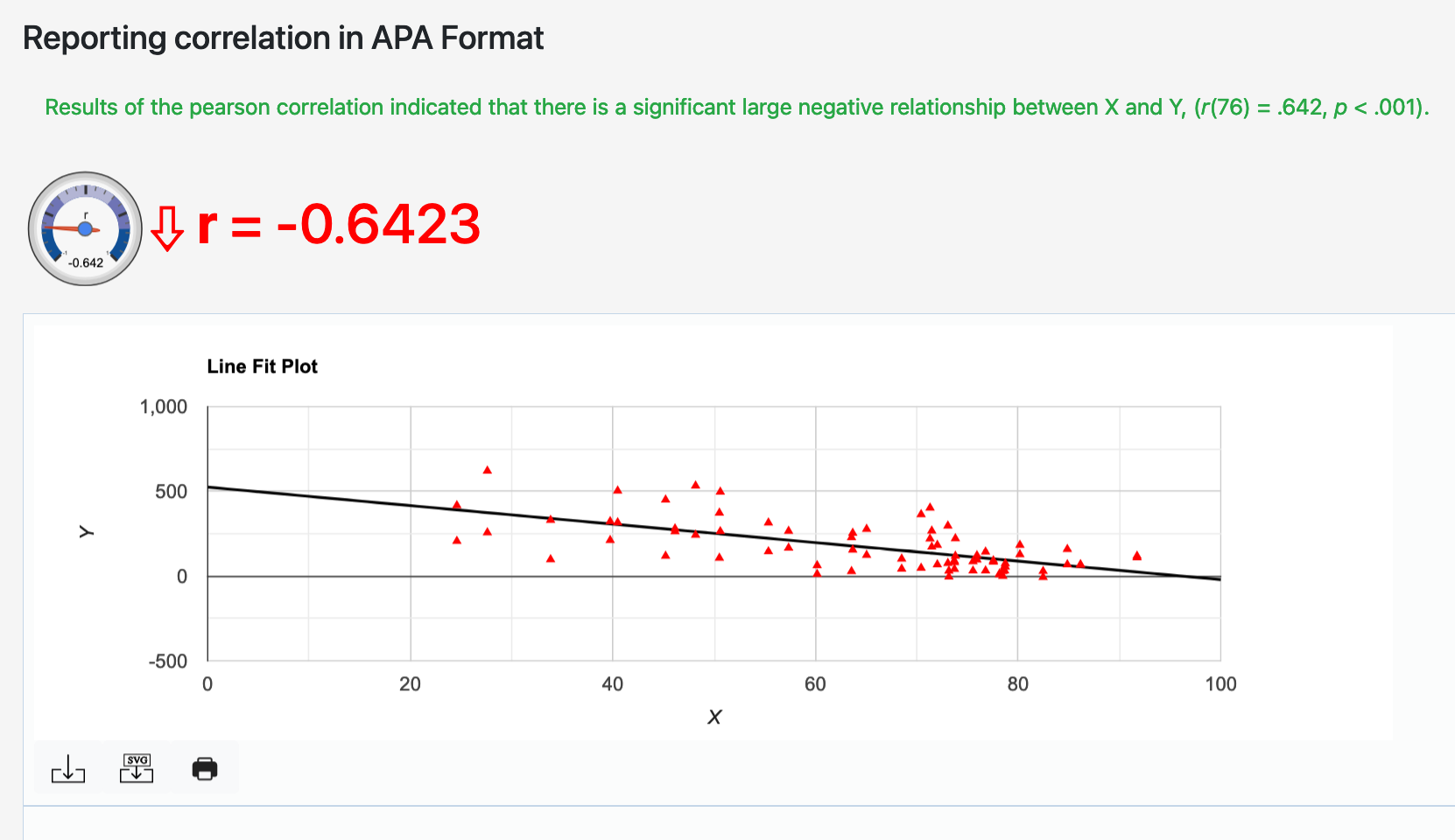
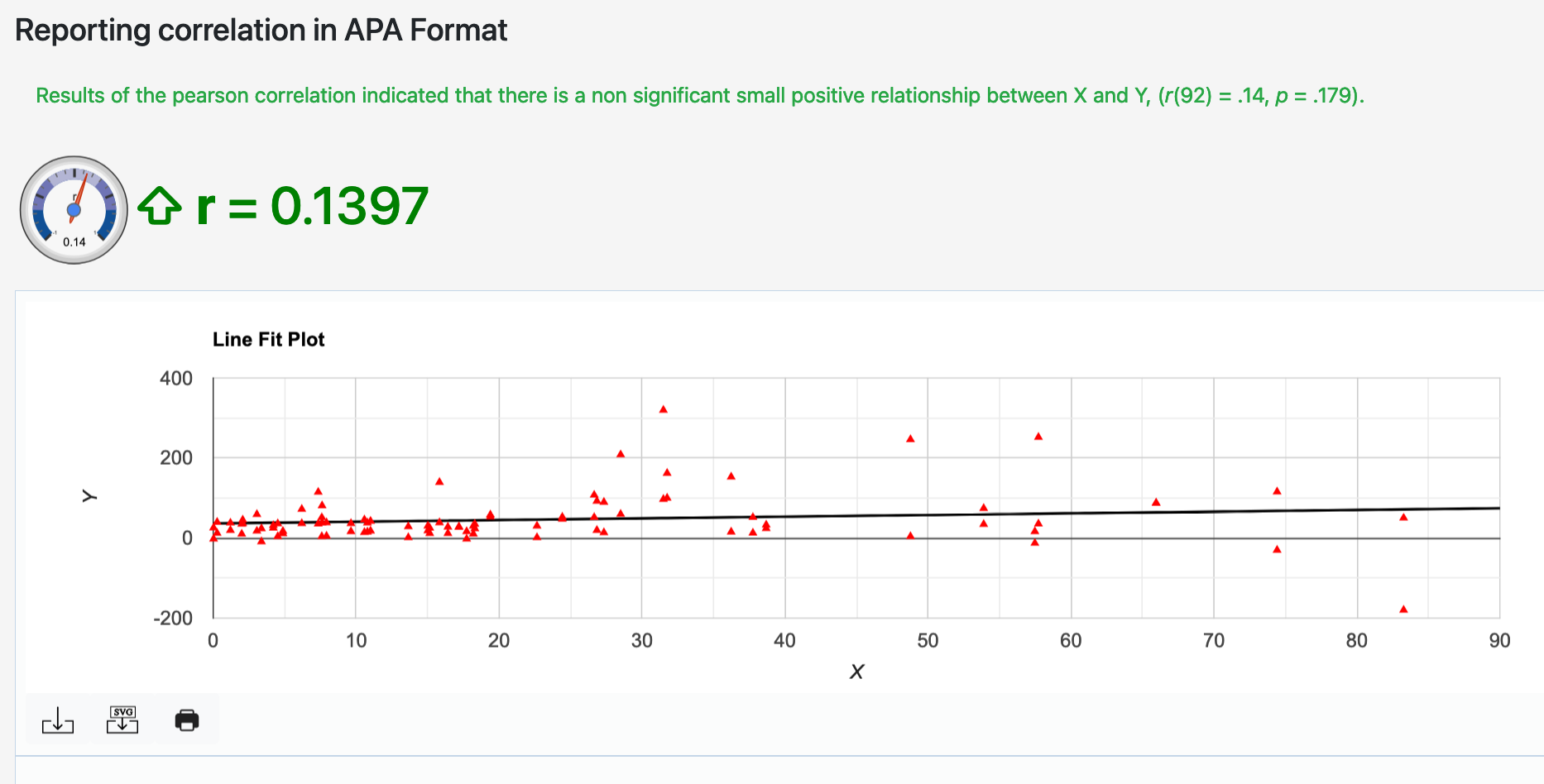
Not only was there no strong negative correlation for Africa, it produced a slightly significant positive correlation - meaning greater rates of vaccination corresponded to greater excess mortality rates!
The vaccine pushers often point out that the median age in Africa is much lower.
But in that case, why is the CDC still recommending COVID19 vaccines for children?
The problems with the Lancet paper
The Lancet paper analyzed v-safe and VAERS data.
v-safe data
First of all, the numbers they have published regarding the v-safe hospitalization rates are completely misleading.

VAERS data
In the case of VAERS, the problem is much worse.
There are follow up death reports which get deleted from VAERS (are they counted in aggregate statistics, or are they not?)

And sometimes VAERS death reports are severely throttled.

And of course, the CDC completely ignores foreign VAERS reports, even though there are over 100 death reports from Japan where a healthcare professional has concluded that the vaccine did cause the death (in the report writeup itself).

So CDC’s claims about death reports in VAERS is incomplete information at best, and outright data obfuscation at worst.
Summary
I still don’t think the COVID19 vaccine caused so many deaths that they could show up in excess mortality statistics. I could be wrong, but till now the data does not emphatically prove that.
But the papers we have seen thus far are not emphatic in the other direction either!
In contrast, I think his analysis of the v-safe dataset is completely wrong
By the way, this is the basic premise of open source software. It is permissionless. For example, I could not have done all my data analysis without the open source spaCy NLP library. And I did not have to submit an IRB to the creators of spaCy and ask for permission to use their software.
Some countries are missing because I wasn’t able to get all the column values.
You investigated this topic so deeply and straightforwardly, I'm now inclined to be open to the possibility that increases in excess deaths might not be vaccine-related. Till now I figured it was a no-brainer that they were.
So I wonder, have you looked into Edward Dowd's supporting evidence for a positive connection between excess deaths and the COVID vaccines? Is it up to your standards? I tried reading his book but got a little turned off by the pageant of (horrific) individual cases. There were many, and they seemed alarming -- but that was probably the intention, more of a sales pitch than evidence. However there were statistical arguments as well. Despite the emotional pandering, which I think was a bad choice, might there still be something to his hypothesis?