

Analysis of New Zealand's COVID19 data
Are there any data discrepancies?

Note: this article is a bit all-over-the-place and does not focus on a specific question. It is mostly intentional, as I want to highlight a few things I am seeing in the hope that people who read this article can add their own insights.
New Zealand reports results from their vaccination campaign here.
VAERS death reports
I looked at the most recent report for the month ending Nov 2022 which was published on 14th Dec 20221.
Here is what it says:
Up to and including 30 November 2022, a total of 184 deaths were reported to CARM after the administration of the Comirnaty vaccine. Following medical assessments by CARM and Medsafe it has been determined that:
163 of these deaths are unlikely related to the COVID-19 vaccine
15 deaths could not be assessed due to insufficient information
2 cases are still under investigation
2 deaths were determined by the Coroner to be due to myocarditis following first dose Covid-19 (Pfizer) vaccination
1 death was likely due to vaccine induced myocarditis (awaiting Coroner’s determination)
for 1 death a link to the vaccine could not be excluded, myocarditis was found at the time of death (this death is awaiting Coroner’s determination).
In other words, of all the death reports after vaccination, no more than 6 of them are considered to be linked to the vaccine.
From the SPLTTYPE field, you will notice that all of these reports are for the Pfizer vaccine. This means NZ does not really have the option to throw non-mRNA vaccines under the bus like Australia recently did:
Australia chose to hide the deaths due to the mRNA vaccines from the public2.

So when I look at the foreign VAERS reports for New Zealand3 , I see a total of 178 deaths which does closely match what has been reported4.
I also added the DERIVED_AGE column so I can do some additional filtering, given that most foreign VAERS reports are missing the age field.
Let us filter this list for same day deaths (NUMDAYS = 0).
There are already 16 such reports.
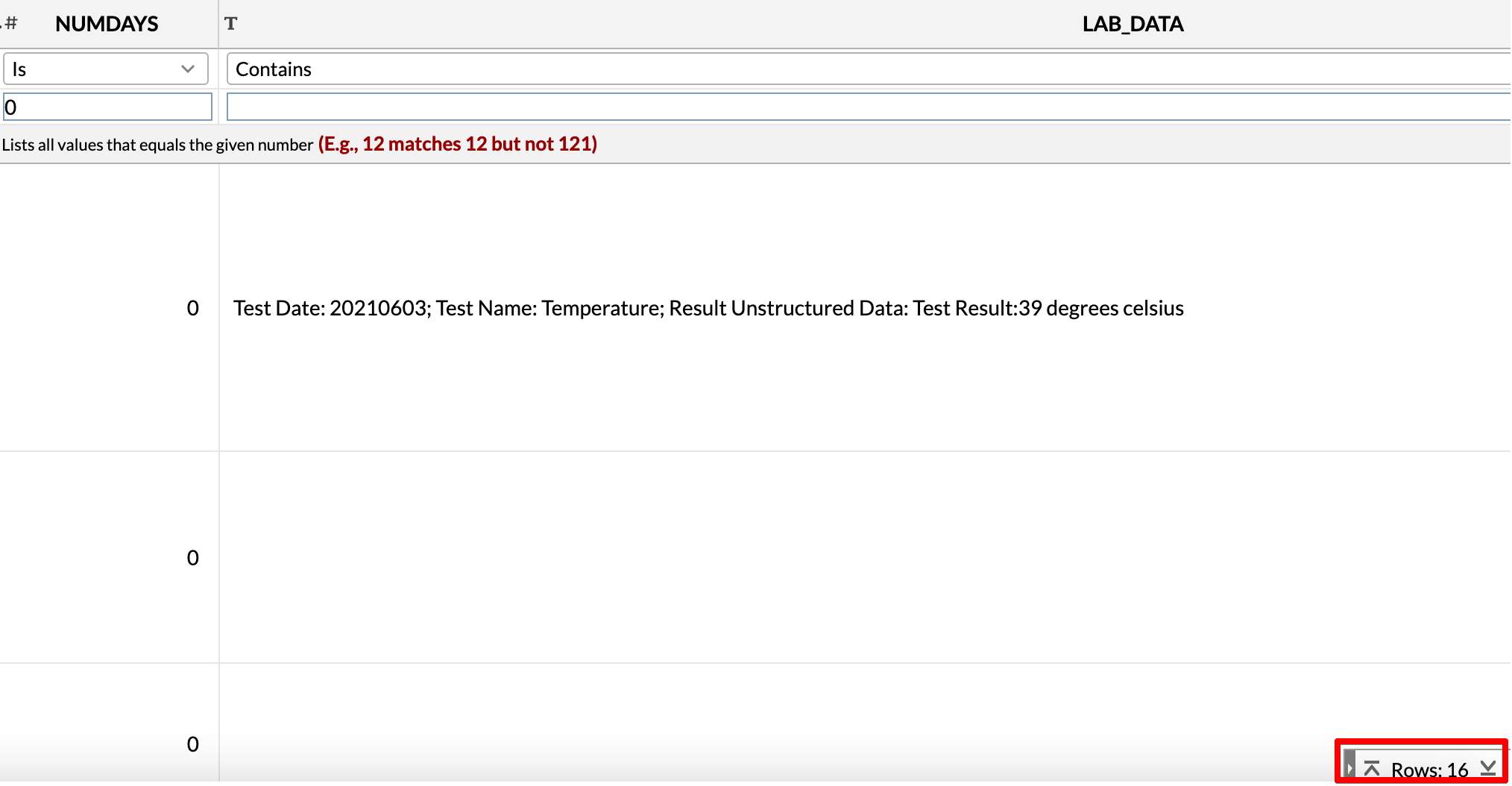
So is the NZ government saying that at most 6 of these were caused by the vaccine?
In case you might be thinking “Well, you are not a medical professional. What makes you think you know better than actual medical professionals?”
Here is an excerpt from the article I cited before (emphasis mine):
Addressing sold out crowds, Dr McCann shared the extraordinary lengths she had to go to to extract causality assessment documents relating to the TGA’s investigation of reported deaths after Covid vaccination, which were obtained under FOI request in a process that took six months. Dr McCann lodged the request after seeing an unexpectedly high number of patients coming through her clinic experiencing adverse events after immunisation (AEFIs). She also noticed a high number of serious AEFI reports in the in the DAEN database, including the reported death of a 14 year old in October 2021.
In her original FOI request, Dr McCann requested causality assessments for all of the reported deaths in the DAEN database. This request was denied due to the large scope, and in negotiation with the TGA, Dr McCann agreed to revise down the request to the 11 documents that were eventually handed over, of which 10 related to DAEN death reports.
When the documents were finally provided to Dr McCann in July 2022, she was dismayed to find that there were multiple reports that the TGA had assessed as causally linked to Covid vaccination, but, with the exception of one death, had not been reported in the TGA’s regular Safety Reports.
So the question is not one of knowledge, but one of trust. I certainly don’t know more than Doctors who are analyzing all these deaths. But I do happen to know that Pfizer made a lot of money from the vaccines, and that the drug regulators in many countries get a lot of their income from the very companies they regulate.
As the TGA is totally funded by industry fees, it is of great importance that its policies on the disclosure and management of conflicts of interest are publicly available
Same with New Zealand
Medsafe is accountable to the Ministry of Health and, through the Ministry, to the Minister of Health. Medsafe is largely funded by fees collected from the therapeutics industry.
Besides, I often wonder how many people have so much as bothered to do a search for VAERS reports from their own countries?
In fact, I don’t think a lot of people are even the slightest bit curious about VAERS, given that people are being continuously told in the media about all the crazy reports, which are probably a very small fraction of the total number.
So back to our analysis.
When you expand to a week, which is well within expected range to attribute to a vaccine, it becomes 78 deaths.
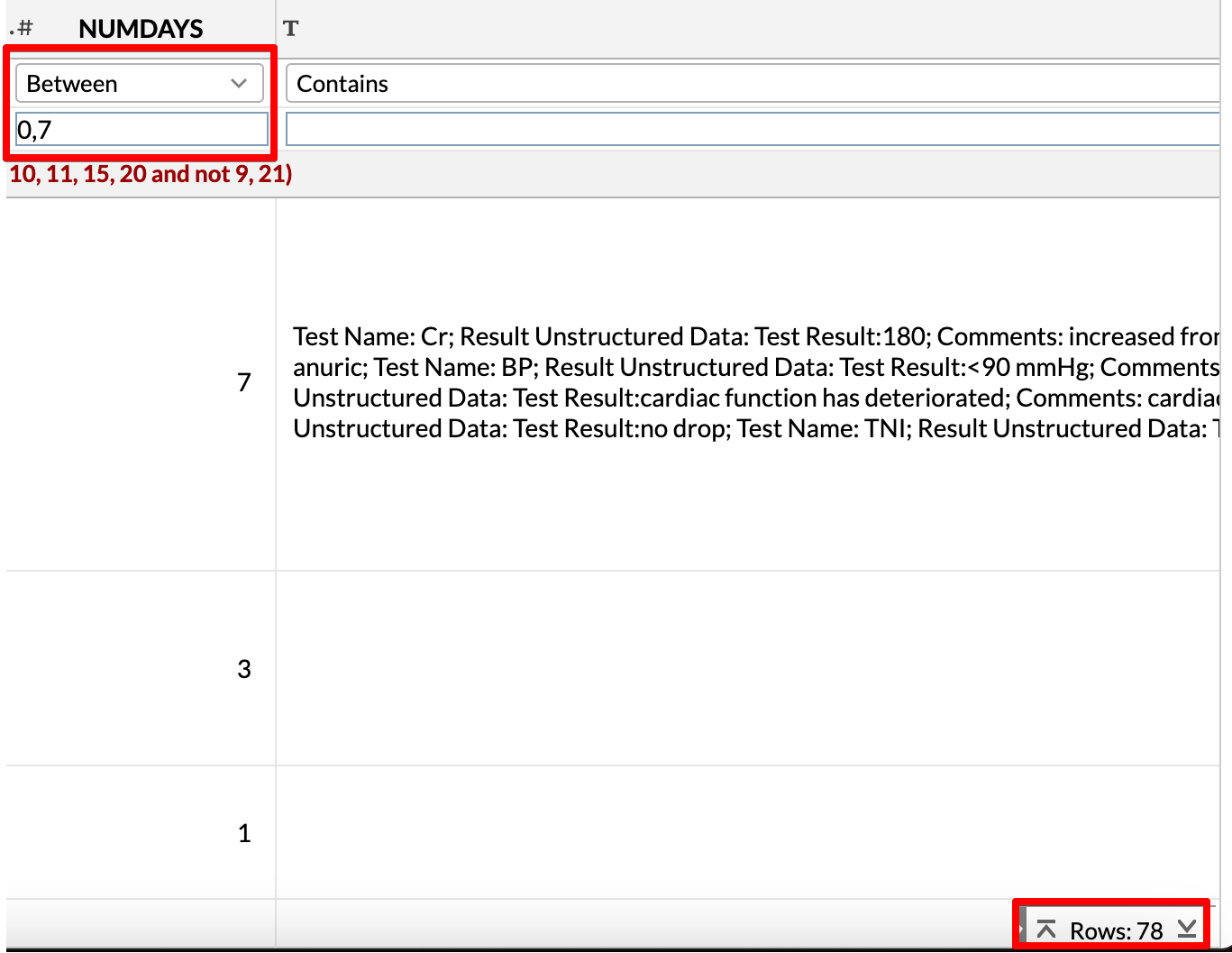
You can also read the narrative text for each report in the SYMPTOM_TEXT column. They are usually quite descriptive.
There are even 26 sudden deaths, of which only 2 happened more than 30 days after vaccination.
All Cause Mortality Data
There was another article published yesterday by Aussie17 (author of
) about New Zealand All Cause Mortality data.
The information was provided only after a FOIA request.
Source (@Bronwyn_Meikle) who requested the data through Official Information Act request. These were not officially published in Stats NZ.
If a government wants to be completely transparent about its vaccination data dashboards, I think they should provide this information up front. Why wouldn’t they just add it into their website without the need for FOIA requests?
This does make me wonder about whether NZ is being fully transparent about the investigation of the death reports.
Booster Doses
The question of booster doses is also very interesting.
A Twitter user replied to my Tweet about this:

So I looked for how many booster doses have been administered in New Zealand.
Turns out, they have administered over 2.75 million booster doses.

But New Zealand’s population is only a little over 5 million. This means they have boosted over 50% of their entire population.
Remember, you can only be boosted AFTER you took dose 1 and dose 2. If you have to also boost over 50% of your population, doesn’t it mean you are already admitting vaccine failure?
Which age group is at highest risk?
Let us also suppose New Zealand only boosted their elderly population, and worked their way down (in terms of age group).
So I downloaded age wise population data for 2022 for New Zealand here.
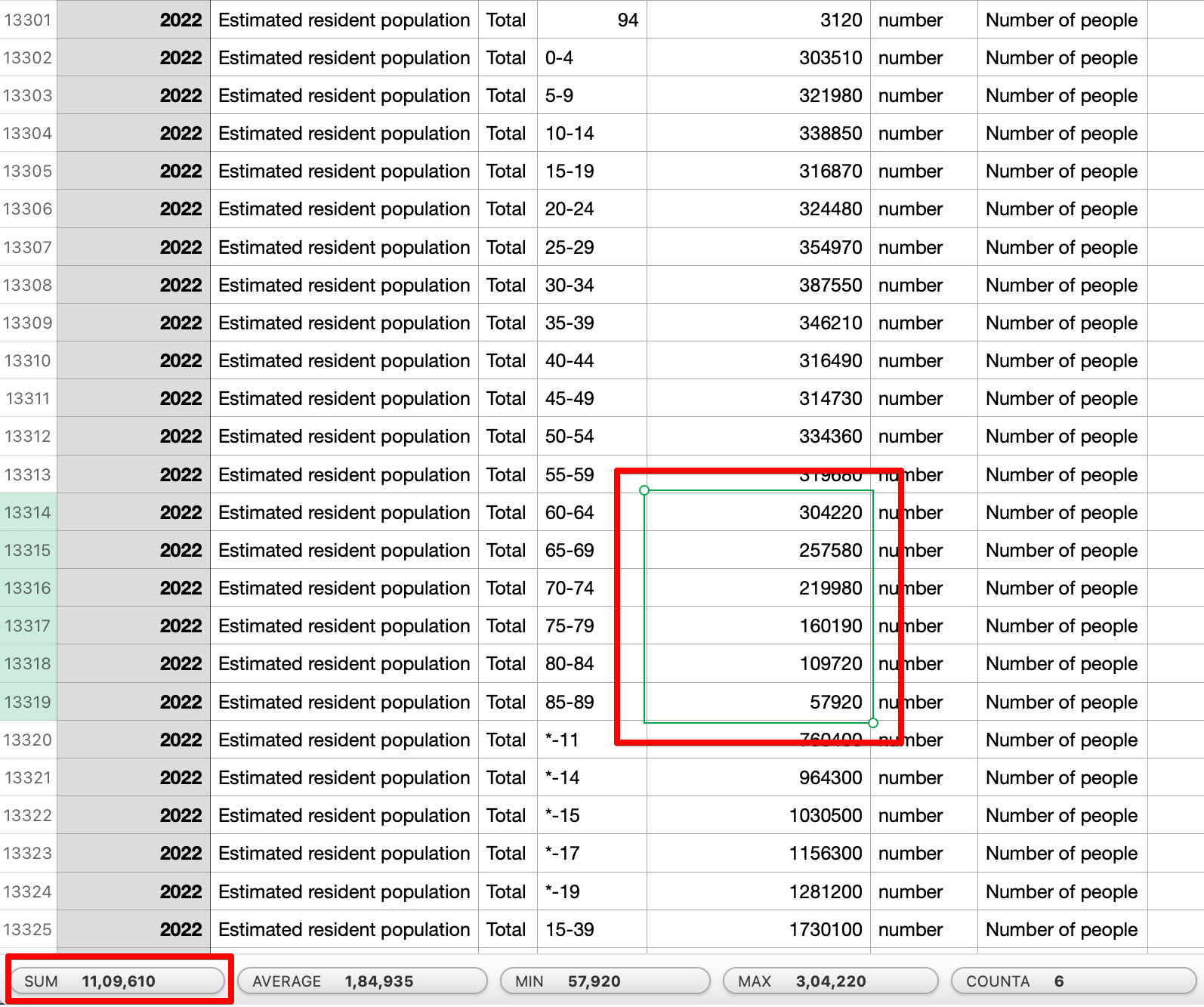
I opened it in a spreadsheet, and started selecting the population column from high → low age groups until I got to about 2.7 million people.
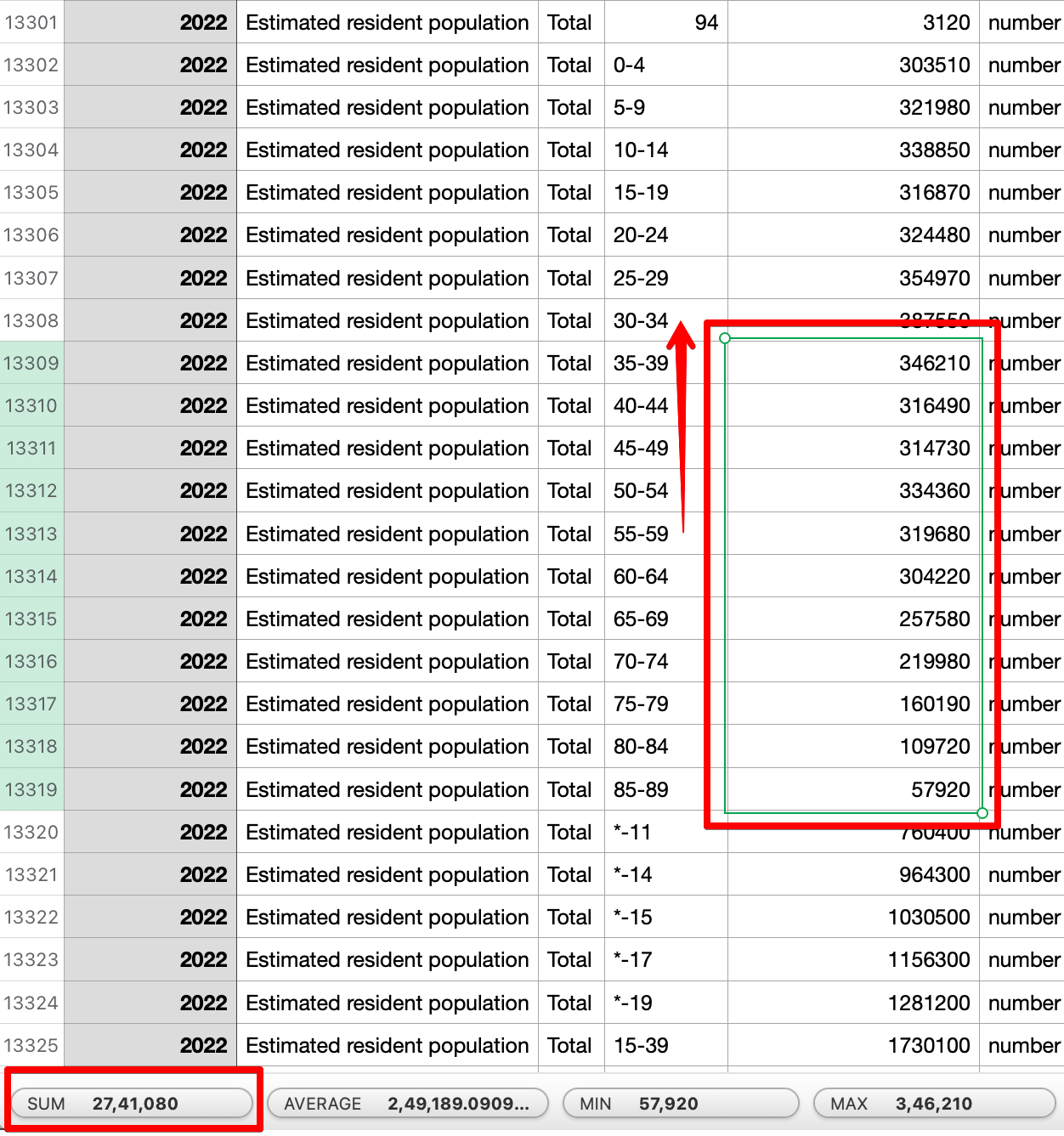
As you can see, the over-60 total population is about 1.1 million people. This still leaves us with over about 1.6 million more.
To do this, they had to vaccinate age groups all the way down to 35-39 at least.
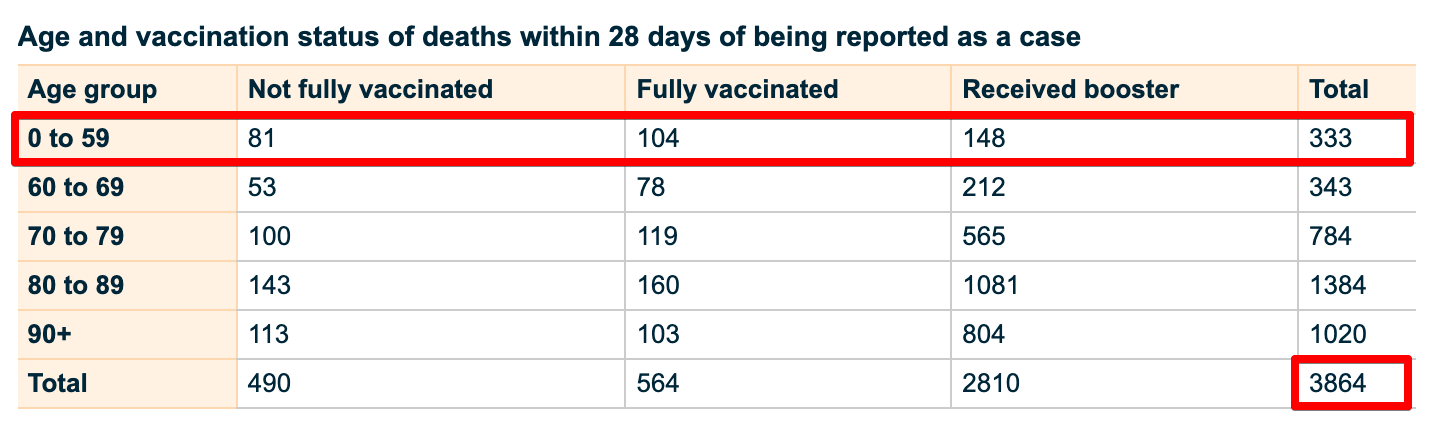
But on their own website you can see that under 60 represented only 10% of the deaths.
In other words, they had to boost a lot of low risk groups (in terms of age).
But if you filter down the VAERS death reports to those which happened within 30 days, you see 31 deaths (And remember, this is based on the DERIVED_AGE field. You would not be able to do this using AGE_YRS because it is often left blank)
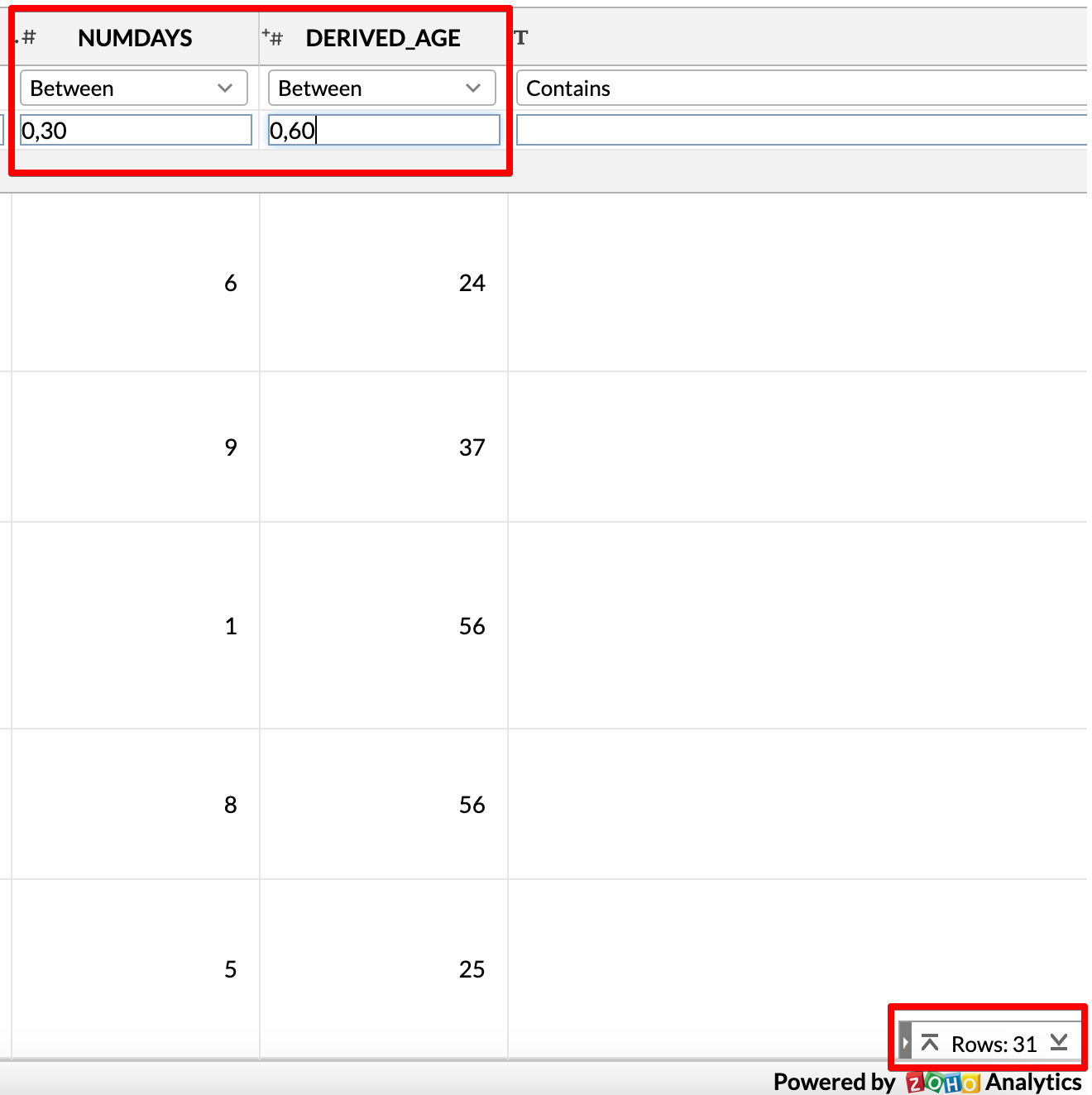
To some, that may look like a reasonable number for a population of 5 million (I personally think it is too high), but that number is actually almost 10% of the total COVID19 deaths for that age group (333)
The website already states that there is a lag of a few weeks
The website VAERSAnalysis.info even compares this to a “limited hangout”
You can filter the data by checking the first two letters in the SPLTTYPE field - for New Zealand it will be NZ
The dataset I used was released around 2nd week of Nov 2022. I used that dataset because it was the last one before CDC started removing narrative text and SPLTTYPE fields citing “privacy” concerns. Since CDC did not intend to make any changes to non-EU and non-UK reports, I believe it is OK for me to reproduce the full reports here.